| Issue |
J Oral Med Oral Surg
Volume 30, Number 3, 2024
|
|
|---|---|---|
| Article Number | 19 | |
| Number of page(s) | 9 | |
| DOI | https://doi.org/10.1051/mbcb/2024020 | |
| Published online | 16 October 2024 | |
Original Research Article
Retrospective study on patient comfort and post-operative condition associated with intravenous sedation versus general anesthesia for third molar extraction in ambulatory surgery in a state hospital
1
Resident in Oral Surgery, Junior Doctor in Lyon's State Hospital Lyon in France
2
Department of Maxillofacial and Stomatology Surgery, Roanne Hospital Centre, 28 rue de Charlieu, 42300 Roanne, France
3
Department of Maxillofacial and Stomatology Surgery, South Lyon Hospital University, University of Claude Bernard Lyon 1, 165 Chemin du Grand Revoyet, 69495 Pierre-Bénite, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
19
February
2024
Accepted:
12
August
2024
Abstract
Objectives: Third molar extraction requires local or general anesthesia. In public hospitals, general anaesthesia is frequently used to perform the most complex extractions and to accommodate patients' wishes. However, the choice of general anesthesia is at the discretion of the care center. Intravenous sedation is also an option. We suggest that comfort and post-operative condition are better in patients undergoing sedation rather than general anesthesia. This study aimed to evaluate the comfort and post-operative condition after third molar extraction in an 18–50-year-old ambulatory surgical population in a state hospital. Method and materials: In the stomatology and maxillofacial surgery department of Roanne Hospital, two anesthetic protocols are used for third-molar extraction. We retrospectively collected 47 patients who underwent third molar extraction between 1st July 2022 and 31st December 2022. Results were collected by questionnaires and data were retrospectively retrieved from medical records. Results: Twenty patients underwent a general anesthesia and twenty-seven underwent intravenous sedation. The study found no difference for the pain level (p < 0.62) between the two anesthesia techniques. The comparison of the approaches indicated that intravenous sedation required a shorter duration of anesthesia (p < 0.0001) and a shorter time in the recovery room (p < 0.0001). Conclusion: This study indicates the feasibility and the effectiveness of intravenous sedation for patients undergoing third molar extraction in a state hospital. As other studies in the literature that have shown greater satisfaction and better recovery in patients undergoing intravenous sedation compared with general anesthesia.
Key words: General anesthesia / intravenous sedation / third molar extraction
© The authors, 2024
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
For over a century, oral and dental surgery has been performed in the office on awake patients. However, with the discovery of ether, the evolution of general anesthesia (GA) and sedative drugs has played a key role in oral surgery, enabling more complex operations to be performed with greater comfort for both patient and practitioner. Sedation anesthesia has evolved in recent years to become a cost-effective and practical method for surgeons, while enabling patients to recover and leave hospital more quickly. There are fewer undesirable effects, but they vary depending on the molecules used for intravenous sedation. Studies in various fields show different benefits of this technique. It may improve the feasibility and the safety of the technique in maxillofacial and oral surgery. In oncology and cardiology, this technique allows a faster recovery time and a quicker discharge from hospital in comparison to anesthesia general after electrochemotherapy of head and neck skin lesions and cryoballon ablation for paroxysmal atrial fibrillation. But the choice of the anaesthesia type is at the discretion of the treatment center [1,2].
Anesthetic techniques used in oral surgery are varied and can be adapted to the patient's needs or clinical situation. They range from non-invasive techniques such as local anesthesia to more complex techniques such as GA [3,4].
Local anesthesia with the addition of adrenaline reduces bleeding through local vasoconstriction [5].
Combining local anesthesia with sedation (LA/S) is intended to reduce patient discomfort. Intravenous sedation is an anesthetic technique used in the operating room. It involves the administration of drugs that induce a slight depression of the central nervous system, while maintaining the patient's spontaneous ventilation, and therefore does not require intubation.
In GA, patient cooperation is no longer an issue, and ventilation is controlled. It is the oldest and most widely used anesthetic operating theatre technique for wisdom teeth avulsion in university public hospitals. Local anesthesia could also be combined with GA to reduce patient discomfort.
Many drugs are used for sedation, with different scheme depending on the anesthetist's protocol. Midazolam and propofol are the drug most commonly used in dental surgery to induce safe sedation. Bispectral analysis can help determine the optimal level of sedation [6–10]. The time spent in the operating room and the recovery phase would therefore be shorter. This could improve patient comfort and satisfaction.
Some studies suggest that local anesthesia with moderate sedation may be better than GA for different reasons like efficiency, a lower incidence of complication, a higher degree of patient satisfaction and a rapid recovery that would allow a safer discharge of the patient [1,11–13]. The objectives of sedation are numerous and vary depending on the point of view of the patient, the surgeon or the anesthetist [14,15].
In public hospitals, GA is frequently used. Depending on the anesthetist preoperative consultation, intravenous sedation become to be more used. We decided to compare anesthetic techniques used in the operating room (GA versus LA/S) for wisdom tooth avulsion in a state hospital. In this study, we will focus on the patient comfort and post-operative condition, as prior endpoint. We postulate that the sedation will improve patient comfort, and will reduce the time spent in the operating room and/or in the post-operative recovery room care (PORRC). Our evaluation will include the potential disadvantages of sedation, such as an increase in pre-operative patient anxiety [16,17]. This pilot retrospective study allowed us to evaluate our hypothesis, before carrying out any more complete, randomized study.
Material and methods
This study received ethical approval from the Ethics committee of the Saint-Etienne General University Hospital, which was registered with the no. UMIN000035594. All methods were performed in accordance with the relevant guidelines and regulations set by the institutional review board.
To compare patient comfort between the two anesthetic techniques, we set up a retrospective study in the Maxillofacial Surgery and Stomatology Department of Roanne Hospital. We evaluated two groups of patients undergoing wisdom teeth avulsion (extraction of 1 to 4 wisdom teeth) in the operating room: a control group receiving GA and a treatment group receiving LA/S.
This study was conducted in a patient population aged between 18 and 50. It is a pilot study, including a minimum of 20 patients in each group, during a data collection of 6 months from 1st July 2022 to 31st December 2022, in a state hospital.
Patients were first seen in consultation by the surgeon, who presented the two types of anesthesia available. Information leaflet for wisdom teeth avulsion were handed to the patient. They decided on the anesthetic technique with the agreement of the anesthetist during the pre-anesthetic consultation. Patients had a cooling-off period corresponding to the time between the consultation with the surgeon and the consultation with the anesthetist. Three surgeons, with the same level of experience, were involved in this study and they all practice the both anesthesia technique.
All patients included in the study were hospitalized for a day and monitored in an ambulatory surgical unit. Written consent to the study was given on discharge. We did not included patients refusing to answer the study questionnaire after surgery, or if they were opposed to the use of their answers and medical data concerning their hospitalization for later scientific research purposes. Were also excluded: minors, and if patients could not choose the type of anesthetic technique for medical reasons.
As primary outcome, we evaluated the patient comfort. In order to compare the patient satisfaction about the anesthesia technique (GA or sedation), they filled up survey questionnaires. Rest of the data were collected from medical records.
The satisfaction survey assessing the patient condition during hospitalization were complete on the day of surgery, before hospital discharge (D0) and also 7 days after the procedure (D7). Two types of questionnaires were used: one for patients who had undergone GA (Appendix 1) and another for patients who had undergone sedation (Appendix 2). The survey measured five dimensions: information understood, preoperative anxiety scale, preoperative comfort scale, visual analogue pain scale and postoperative complications. Patients undergoing sedation had also a second questionnaire to fill out concerning their experience during the operation [18].
As secondary outcomes, we studied the post-operative complications, the time spent in the operating room, time spent in the PORRC and anesthesia duration. For GA, anesthesia duration was from intubation to extubation. For sedation, anesthesia duration began with the first administration of sedative drugs and ended with the last dose. These data were retrospectively retrieved from anesthesia records. Patient's follow-up by medical records for post-operative complications was set at 30 days from the date of surgery. Of the patients collected, 27 chose sedation anesthesia and 20 chose general anesthesia.
Before surgical incision, all patients received an injection of 2 grams of amoxicillin, 40 milligrams (mg) of methylprednisolone, 100 mg of ketoprofen (100 mg/4 mL ampoule) and 15 mg/kg of paracetamol.
The GA and sedation protocol are shown in the following tables (Tab. I). Patients under sedation received fewer hypnotic drugs than patients under GA. Patients in both groups also received ropivacaïne during the procedure. Patients under sedation received local anesthesia with 1/200,000 adrenalized articaïne for wisdom teeth avulsion [5,6,19].
Patients in both groups were discharged from hospital with the following prescription: Prednisolone 20 mg, 2 tablets in the morning for 3 days; paracetamol 500 mg, 2 tablets every 6 hours for 5 days; chlorhexidine digluconate solution 0.2%, mouthwash solution, 200 mL bottle, 1 mouthwash after every meal for 7 days; and a surgical toothbrush.
The qualitative variables, expressed as percentages, were compared by a Mann-Whitney test. The numerical variables, expressed as mean + SD (Standard Deviation), were compared by a Fisher test. All statistical tests were two-tailed, and the significance level was set at 5% (alpha at 5%).
Results
Population
Our sample consists of two comparable groups for the variables of sex, age and number of wisdom teeth extracts. However, there was a statistically significant difference (p<0.0001) for the level of education variable (Tab. II). There is any medical conditions found in the two groups. None patient had any comorbidity, they were nonsmokers. We found that patients opting for sedation generally had a higher level of education than those opting for GA.
Anesthesia protocol for different anesthetics.
Information
At the first consultation with the surgeon, 80% of the GA-group patients preferred GA and 20% had no preference (p < 0.0005). In the LA/S group, 58% had no preference for the type of anaesthesia and 23% preferred GA (Tab. III). Most patients were not aware of the existence of sedation or did not know what it was. In the GA group, 13 patients preferred it because they were scared by the atmosphere of an operating room. Information on the different types of anesthesia explained and seems to be understood by all patients included in the study.
Population characteristics.
Patient status/comfort before surgery
The evaluation of patient anxiety was compared: 70% of patients in the LA/S group had a mild or no anxiety, and 65% of patients in the GA group had moderate/severe anxiety (p < 0.08). There were no statistical differences (p < 0.68) between groups in terms of waiting time in the ambulatory surgery unit (Tab. IV). One patient in each group experienced discomfort while waiting in the operating room.
Information on different types of anesthesia.
Patient comfort after surgery
There were no significant differences in pain level (p < 0.62) among patients in the outpatient surgery unit (Tab. V). However, 47% of patients in the LA/S group had the same pain level less than 4 hours and more than 4 hours after surgery. In the GA group, 50% complained directly after surgery. Overall, patients were satisfied with the type of anesthesia chosen (96% satisfied in the LA/S group and 100% satisfied in the GA group). There was no loss of sensitivity in the lip or tongue, and no dental trauma following intubation or surgery.
Assessment of anxiety before surgery.
During surgery in the LA/S group
In this group, patients were asked to complete an additional questionnaire assessing their experience during the procedure (Appendix 2).
These patients were generally confident in the type of anesthesia proposed (88%) and they were not scared that the sedation would not take effect. Patients had a generally pleasant memory of the sedation procedure (66%), while the remainder had no memory at all. In this group, 23 patients experienced no discomfort, 2 experienced pain at the surgical site, 2 experienced pain at the IV catheter site during the passage of drugs and 1 felt cold during the procedure (Fig. 1).
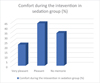 |
Fig. 1 Comfort during the intervention in sedation group (%). |
At D7 post-op
Few patients responded to their questionnaires at 1 week post-op: 7 questionnaires were returned in the LA/S group and 4 in the GA group. No analysis could be carried out given the insufficient number of responses.
Patient management times
We observed a significant difference in anesthesia times (p < 0.0001) and time spent in the PORRC (p < 0.0001). The duration of anesthesia was reduced for the LA/S group, with an average of 34 min, compared with an average of 64 min for GA (Tab. VI). The time spent in the PORRC was also shorter in the LA/S group, with an average of 16 min versus 80 min for GA. Operating time remained similar between the two groups, with an average of 25 min for LA/S and 28 minutes for GA.
Patient comfort after surgery at Day 0.
Comparison of anesthesia, operating and recovery times between the two groups
Post-operative and emergency follow-up
The number of patients who returned was 5 (25%) in the GA group and 7 patients (25%) in the LA/S group. They returned for alveolitis, pain or swelling. No statistical analysis could be performed.
Discussion
The aim of this study was to evaluate 2 different anesthetic techniques and the comfort of patients undergoing third-molar extraction in a state hospital. In addition, we analyzed the operative and recovery times. Third molar extraction can be performed under local anesthesia, continuous intravenous sedation or general anesthesia, but there are no standardized anesthetic protocols in state hospital [20].
This study, evaluating post-operative patient experience as the prior end points, found no difference in pain evaluation (p < 0.62). However, patients in the LA/S group complained of pain more than 4 hours after surgery (47%), unlike patients who underwent GA, who complained of pain directly in the operating room (50%). This statistical difference (p < 0.03) in temporality can be explained by the local anesthetics used during surgery. The short half-life of adrenalized articaïne would explain the delayed pain sensations in the LA/S group. This result highlights the benefit of given local anesthesia. We would recommend to used it as well for procedure under GA, to reduce the immediate postoperative pain.
The study showed a significant difference on the secondary endpoints of anesthesia time (p < 0.0001) and time spent in the PORRC (p < 0.0001). Indeed, anesthesia time was reduced for the LA/S group, with an average of 34 min versus 64 min for GA. Patients who were less soaked by hypnotic drugs recovered more quickly than patients who had to be extubated after GA. This explains the shorter recovery time in the LA/S. Operating time remained more or less the same between the two groups, with an average of 25 min for LA/S and 28 min for GA.
A study analyzing adverse anesthesia outcomes in 1 180 ambulatory oral surgery patients, found similar results. In this study of Epy Chye [13], the incidence of pain in post-operative was the same with 66% of pain in GA group and 66% in LA/S. The mean recovery time sit in minutes was 61 minutes for GA and 38 minutes for moderate sedation. The incidence of post-operative nausea and vomiting during recovery was 6% for subject receiving moderate sedation and 14% for subjects receiving GA.
Our study showed no difference between the two techniques in terms of post-operative follow-up. In the prospective study by Inverso et al. [21], there wasn't more complication associated with GA than with sedation. In their study, the preoperative anxiety score increased the perioperative anesthetic risk by 23 % per level of increase complication. Methods to reduce the anxiety of patients undergoing surgery have been shown to decrease the rate of perioperative and postoperative complications. In our study, anxiety was higher in the GA group (65%) than LA/S (30%).
The study by Sammut et al. [22], shows a trend in the choice of anesthesia type depending on the facility where patients undergo surgery. A hospital specialized in oral surgery is more likely to offer local anesthesia or sedation than GA. On the other hand, a hospital dedicated to oral and maxillofacial surgery will offer more tooth extractions under GA, without any link to the difficulty of each case. This depends on the structure and experience of the practitioners. They also noted a socio-economic difference in the choice of anesthesia as in our study with the level of education. Eighty-one % of the LA/S patients had an advanced degree of education versus 40% in GA (p < 0.0001).
According to the study by Craig et al., sedation can be used in oral surgery for long operations to imporve patient comfort. If the surgery lasts longer than 90 minutes, e.g. in the case of a complex implant procedure, sedation can be useful. It avoids making the procedure unpleasant for the patient, as standing still for long time with the mouth open can be difficult for a fully conscious patient [23].
More recent studies have indicated the feasibility and safety of continuous intravenous sedation compared to GA for patients undergoing electrochemotherapy of cutaneous tumour nodules. Indeed, a lower dosage of propofol during continuous intravenous sedation is advantageous for patients in order to speed up recovery time and allow discharge from hospital [24,25]. Moreover, dental procedures are less invasive and do not generally affect the speed of recovery and discharge times, unlike general surgery, where the effects of procedures can significantly affect recovery and discharge [26].
Some studies show that we can go even further with sedated patients. As patients are conscious throughout the procedure, other relaxation methods can be combined with sedation. Indeed, the study by Mackey et al. [27,28], showed that combining sedation with hypnosis or suggestion therapies could reduce the amount of sedative drugs used during the procedure. This would reduce the risks of complication associated with these drugs, as well as their cost. Hypnosis also appears to reduce post-operative pain and painkiller consumption and thus improve the satisfaction [29]. These finding suggest that reduce postoperative pain enable to reduce pain reliever consumption.
In terms of population characteristics, we noted a difference in patients' level of education between the two groups. Patients opting for sedation generally had a higher level of education, unlike patients choosing GA. Sedation was better understood by patients with higher levels of education, demonstrating the importance of patient understanding and communication during the consultation with the surgeon and anesthetist.
The results of our study must be considered in the light of various limitations. This pilot study enrolled a total of 47 patients, which may explain the study's lack of power. It would be interesting to carry out the same protocol on a larger scale, prospectively. This would probably enable more precise and narrower results to be obtained. Another bias of our study is that patients had the choice of their anaesthesia technique. A more large-scale randomized study should be done in order to assess the patient comfort before/during and after sedation regardless of the character of the subject. The dosage of the drugs used was not recorded in the data set and also this could have influenced the incidence of post-operative complications. Many various intravenous drugs are found in the literature and comparison between all intravenous drugs is difficult. The anesthesia protocol remains at the discretion of the anesthetist's team.
Conclusion
In conclusion, despite the limitations, the pilot-study has demonstrated that the post-operative comfort is not different between the sedation and general anesthesia for patient undergoing third molar extraction in a state hospital. Overall satisfaction was high in both arms. The time spent in the recovery room after intravenous sedation is shorter than general anesthesia group. Future studies should consider a larger population to evaluate the postoperative condition, operative time and recovery time. Some evidence suggests that sedation may be better than general anaesthesia if care is taken to administer effective intra-operative dose. Patient satisfaction can be achieved in a large public teaching hospital through sedation. In addition, a faster recovery time allows earlier discharge from the hospital and may be beneficial for patient satisfaction and comfort and also for hospital costs.
Supplementary material
Appendix 1. Satisfaction survey to assess patient condition during hospitalization after third molar extraction under general anesthesia.
Appendix 2. Satisfaction survey to assess patient condition during hospitalization after third molar extraction under sedation.
Access Supplementary MaterialAcknowledgments
This research did not receive any specific funding.
Funding
There is no funding for this study.
Conflicts of interest
The authors declare that they have no conflict of interest.
Data availability statement
The data will be made available upon reasonable request.
Author contribution statement
Dr. Légroz Eloïse: Design of methodology, conducting the research, collecting data, analyse study data, writing and revision.
Dr. Petre Lupu Bratiloveanu: Statement of hypothesis, conducting the research.
Dr. Andréa Varazzani: Revision.
Informed consent
Written informed consent was obtained from all patients and/or families.
References
- Kramer KJ, Ganzberg S, Prior S, et al. Comparison of propofol-remifentanil versus Propofol-Ketamine deep sedation for third molar surgery. Anesth Prog 2012;59:107–117. [CrossRef] [PubMed] [Google Scholar]
- Sebastiani FR, Dym H, Wolf J. Oral sedation in the dental office. Dent Clin North Am 2016;60:295–307. [CrossRef] [PubMed] [Google Scholar]
- Arreto C-D. Anesthésiques locaux. Arreto CD Anesth Locaux EMC − Médecine Buccale 20161121-14Article 28-185-M-10 2016; https://www.em.premium.com/article/1097898/resultatrecherche/13 (updated 2016; consulted 2023-01-19) doi:10.1016/S0000-0000(08)53167-6. [Google Scholar]
- Molliex S, Plaud B, Sammain E, et al. Medecine intensive, réanimation, urgences et défaillances viscérales aiguës. Collège National des enseignants d'anesthésie et de réanimation (CNEAR), Elsevier Masson. 2021, pp 85–103. [Google Scholar]
- Bennaceur S, Sagnet P, Ernewein D, et al. Anesthésies locale, locorégionale et générale en odontologie et stomatologie pédiatriques. Selim Bennaceur Pierre Sagnet Didier Ernewein Christine Maudier Samie Louafi Gérard Couly Anesth Locale Locorégionale Générale En Odontol Stomatol Pédiatriques EMC − Odontol 20011–15 Artic 23-400-G-10 https://www.em.premium.com/article/20551/resultatrecherche/5 (updated 2001; consulted 2023-01-19). [Google Scholar]
- Kramer KJ, Brady JW. Anesthetic agents commonly used by oral and maxillofacial surgeons. Oral Maxillofac Surg Clin N Am 2018;30:155–164. [CrossRef] [Google Scholar]
- Jackson DL, Johnson BS. Inhalational and enteral conscious sedation for the adult dental patient. Dent Clin North Am 2002;46:781–802. [CrossRef] [PubMed] [Google Scholar]
- Rai K, Hegde AM, Goel K. Sedation in uncooperative children undergoing dental procedures: a comparative evaluation of midazolam, propofol and ketamine. Clin Pediatr Dent 2007;32:1–4. [Google Scholar]
- Sandler NA, Sparks S. The Use of Bispectral Analysis in Patients Undergoing Intravenous Sedation for Third Molar Extractions J Oral Maxillofac Surg 2000;58:364–368. [Google Scholar]
- Moore PA, Nahouraii HS, Zovko JG, Wisnieski SR. Dental therapeutic practice patterns in the U.S.I. Anesthesia and sedation. 2006. [Google Scholar]
- Corcuera-Flores J-R., Silvestre-Rangil J, Cutando-Soriano A et al. Current methods of sedation in dental patients − a systematic review of the literature. Med Oral Pathol Oral Chirugia Bucal 2016. doi:10.4317/medoral.20981. [Google Scholar]
- Ganzberg S, Pape RA, Beck FM. Remifentanil for use during conscious sedation in outpatient oral surgery. J Oral Maxillofac Surg 2002;60:244–250. [CrossRef] [PubMed] [Google Scholar]
- Chye EPY, Young IG, Osborne GA, et al. Outcomes after same-day oral surgery: a review of 1,180 cases at a major teaching hospital. J Oral Maxillofac Surg 1993;51:846–849. [CrossRef] [PubMed] [Google Scholar]
- Edwards DJ, Brickley MR, Edwards MJ, et al. Choice of anaesthetic and healthcare facility for third molar surgery. Br J Oral Maxillofac Surg 1998;36:333–340. [CrossRef] [PubMed] [Google Scholar]
- Jacquens A, Simony M, Besnard A, et al. Surveillance de la profondeur d'anesthésie générale. Wwwem-Premiumcomdatatraitesan 36–59002 https://www.em.premium.com/article/1561671 (updated 2022; consulted 2023-01-19) doi:10.1016/S0246-0289(22)59002-7. [Google Scholar]
- Garip H, Gürkan Y, Toker K, et al. A comparison of midazolam and midazolam with remifentanil for patient-controlled sedation during operations on third molars. Br J Oral Maxillofac Surg 2007;45:212–216. [CrossRef] [PubMed] [Google Scholar]
- Esen E, Üstün Y, Balcıoğlu YO, et al. Evaluation of patient-controlled remifentanil application in third molar surgery. J Oral Maxillofac Surg 2005;63:457–463. [CrossRef] [PubMed] [Google Scholar]
- Holland IS, Stassen LF. Bilateral block: is it safe and more efficient during removal of third molars? Br J Oral Maxillofac Surg 1996;34:243–247. [CrossRef] [PubMed] [Google Scholar]
- Lemogne M, Bouley D, Buscail D, et al. Anesthésie en stomatologie et en chirurgie maxillofaciale. Michaël Lemogne Daniè Bouley Didier Buscail Henriette Falkman Laurent Jacob Anesth En Stomatol En Chir Maxillofac EMC − Anesth-Réanimation 1992 1-0 Artic 36-615-C-10. [Google Scholar]
- Haute Autorité de santé. Avulsion des 3ème molaires: indications, techniques et modalités. 2019 (updated 2019; consulted 2023-06-30). [Google Scholar]
- Inverso G, Dodson TB, Gonzalez ML, et al. Complications of moderate sedation versus deep sedation/general anesthesia for adolescent patients undergoing third molar extraction. J Oral Maxillofac Surg 2016;74:474–479. [CrossRef] [PubMed] [Google Scholar]
- Sammut S, Lopes V, Morrison A, et al. Predicting the choice of anaesthesia for third molar surgery − guideline or the easy-line? Br Dent J 2013;214:E8–E8. [CrossRef] [PubMed] [Google Scholar]
- Craig DC, Boyle CA, Fleming GJP, et al. A sedation technique for implant and periodontal surgery. J Clin Periodontol 2000;27:955–959. [CrossRef] [PubMed] [Google Scholar]
- Benedik J, Ogorevc B, Brezar SK, et al. Comparison of general anesthesia and continuous intravenous sedation for electrochemotherapy of head and neck skin lesions. Front Oncol 2022;12:1011721. [CrossRef] [PubMed] [Google Scholar]
- Wasserlauf J, Kaplan RM, Walega DR, et al. Patient‐reported outcomes after cryoballoon ablation are equivalent between moderate sedation and general anesthesia. J Cardiovasc Electrophysiol 2020;31:1579–1584. [CrossRef] [PubMed] [Google Scholar]
- Lepere AJ, Slack-Smith LM. Average recovery time from a standardized intravenous sedation protocol and standardized discharge criteria in the general dental practice setting. Anesth Prog 2002;49:77–81. [PubMed] [Google Scholar]
- Mackey EF. Effects of hypnosis as an adjunct to intravenous sedation for third molar extraction: a randomized, blind, controlled study. Int J Clin Exp Hypn 2009;58:21–38. [CrossRef] [Google Scholar]
- Mackey EF. An extension study using hypnotic suggestion as an adjunct to intravenous sedation. Am J Clin Hypn 2018;60:378–385. [CrossRef] [PubMed] [Google Scholar]
- Coyle TT, Helfrick JF, Gonzalez ML, et al. Office-based ambulatory anesthesia: factors that influence patient satisfaction or dissatisfaction with deep sedation/general anesthesia. J Oral Maxillofac Surg 2005;63:163–172. [CrossRef] [PubMed] [Google Scholar]
Cite this article as: Légroz E, Bratiloveanu PL, Varazzani A. 2024. Retrospective study on patient comfort and post-operative condition associated with intravenous sedation versus general anesthesia for third molar extraction in ambulatory surgery in a state hospital. J Oral Med Oral Surg, 30: 19. https://doi.org/10.1051/mbcb/2024020
All Tables
All Figures
|
Fig. 1 Comfort during the intervention in sedation group (%). |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.