| Issue |
J Oral Med Oral Surg
Volume 32, Number 1, 2026
|
|
|---|---|---|
| Article Number | 2 | |
| Number of page(s) | 5 | |
| DOI | https://doi.org/10.1051/mbcb/2026005 | |
| Published online | 17 March 2026 | |
Case Report
Iatrogenic osteomyelitis in patients with florid cemento-osseous dysplasia: an illustrative case report
1
Department of Oral and Maxillofacial Surgery, University Hospital of Caen, Caen, France
2
Department of Oral Medicine and Oral Surgery, CHU Rouen, Rouen, France
3
Department of Oral Medicine and Oral Surgery, Bretonneau Hospital, Paris, France
4
UFR d’Odontologie, Faculté de Santé, Université Paris Cité, F-75006 Paris, France
5
Laboratory of Orofacial Neurobiology, EA 7543, Université Paris Cité, F-75006 Paris, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
18
September
2025
Accepted:
19
January
2026
Abstract
Introduction: Cemento-osseous dysplasia (COD) is a benign fibro-osseous lesion of the jaws, often asymptomatic but potentially complicated by secondary infection due to its hypovascular nature. Osteomyelitis may occur following minor trauma or dental procedures when the condition is unrecognized or improperly managed. Case report: A 52-yr-old woman of African descent developed osteomyelitis of the right mandible after multiple tooth extractions performed abroad. CBCT imaging revealed bilateral florid COD with mixed radiolucent–radiopaque lesions and bone sequestra. Conservative surgical debridement under local anesthesia, followed by prolonged antibiotic therapy, allowed symptom resolution, full mucosal healing, and bone remodeling. Discussion: This case illustrates the iatrogenic risk of invasive procedures in unrecognized COD. The hypovascular, sclerotic bone limits healing and antibiotic diffusion, predisposing to chronic infection. Previous reports similarly describe secondary osteomyelitis arising in florid COD and support conservative management combining limited debridement and prolonged antibiotic therapy. Early radiographic recognition and pulp vitality testing of teeth with unexplained periapical radiolucencies are key to preventing misdiagnosis. When infection occurs, conservative management, when possible, ensures optimal outcomes. Conclusion: Clinicians should suspect COD in middle-aged women of African descent presenting with mixed mandibular lesions. Early diagnosis and avoidance of unnecessary extractions can prevent osteomyelitis and reduce morbidity.
Key words: Cemento-osseous dysplasia / florid cemento-osseous dysplasia / osseous dysplasia / osteomyelitis
© The authors, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Cemento-osseous dysplasia (COD) is a benign fibro-osseous lesion characterized by the replacement of normal bone with fibrous tissue and cementum-like or immature bone deposits [1]. The World Health Organization classified COD into four distinct subtypes : periapical, typically localized to the anterior mandible; focal, typically localized in the posterior regions of the jaws; florid, being multifocal and bilateral (or often symmetrical); and familial gigantiform cementoma [2]. The prevalence of COD varies considerably among populations. In general radiographic screenings, it is estimated at less than 1% of cases but may rise to approximately 5.5% in individuals of African descent, where it predominantly affects middle-aged women [2,3]. Florid COD represents approximately 45% of COD cases and is most prone to secondary infection due to its hypovascular, multifocal nature [4].
Although often asymptomatic and discovered incidentally on radiographs, COD is frequently misdiagnosed as periapical pathology, prompting unnecessary endodontic treatment or extractionsboth of which can precipitate osteomyelitis. Indeed, the hypovascular dysplastic lesions impair antibiotic diffusion and bone healing, with the risk of chronic osteomyelitis development [5].
This article aimed to present an illustrative case report of iatrogenic osteomyelitis following dental extractions in a patient with florid COD and discuss the relevant literature.
Case report
A 52-yr-old woman of African descent was referred to the dental emergency department in January 2024 for pain and swelling in the right mandibular region (teeth 46–48). Symptoms began one month after extractions of teeth 46, 47, and 48, performed four months earlier abroad, due to persistent dental pain. The initial radiograph was unavailable, and prior endodontic treatment status was unknown.
Her medical history included hypertension (treated with nicardipine hydrochloride) and well-controlled type 2 diabetes (managed with metformin). She was a non-smoker, reported no alcohol consumption, and had no known allergies.
Extraoral examination was normal. Intraoral examination revealed swelling, localized gingival hypertrophy, and purulent discharge in the right posterior mandible (Fig. 1). No neurosensory alterations in the territory of the right inferior alveolar and mental nerves were observed. A cone beam computed tomography (CBCT) scan showed a 4-cm lobulated lesion with mixed radiolucent and radiopaque areas, sclerotic changes, and bone sequestra in the right mandible (Fig. 2). The contralateral side of the mandible (area 3) showed features suggestive of florid COD (Fig. 3).
The working diagnosis was florid COD with secondary infectious osteomyelitis. Differential diagnoses included chronic diffuse sclerosing osteomyelitis, ossifying fibroma, and idiopathic osteosclerosis. Histopathological confirmation was planned post-surgery.
Following multidisciplinary consultation, conservative surgical management was decided, consisting of debridement of necrotic tissue and sequestrectomy under local anesthesia, with histopathological analysis of harvested specimens, combined with antibiotic therapy. The goals were to remove necrotic tissue, reduce bacterial load, and preserve viable bone.
Patient information (and subsequent informed consent) emphasized infection and healing risks due to underlying COD.
Surgery was performed two weeks later using 4% articaine with low-dose epinephrine (1/200000). Amoxicillin/clavulanic acid (1 g twice daily) was prescribed postoperatively for three weeks until mucosal healing. The excised specimen was submitted for histopathology to confirm the diagnosis and rule out other bone diseases, notably malignant conditions (Fig. 4).
At the three-week follow-up, mucosal healing was complete, with no pain or inflammation. Histopathology revealed sclerotic, devitalized bone, consistent with osteonecrosis without neoplastic features, granulation tissue, or microbial colonies.
A four-month follow-up CBCT showed osseous remodeling in the right mandible. A residual radiodense area likely represented post-surgical healing or persistent COD (Fig. 5). The mucosa remained intact, with no fistula, suppuration, or pain. Biannual clinical and radiographic follow-up was planned to monitor for potential recurrence or secondary infection. The patient declined prosthodontic rehabilitation.
 |
Fig. 1 Intraoral view showing swelling and purulent discharge in the right posterior mandible. |
 |
Fig. 2 CBCT scan depicting mixed radiolucent-radiopaque lesions with bone sequestra in the right mandible. A: sagittal view. B: coronal view. C: 3D reconstruction. |
 |
Fig. 3 CBCT panoramic reconstruction illustrating bilateral mandibular involvement with mixed radiolucent and radiopaque areas, typical of florid COD. |
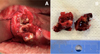 |
Fig. 4 A: endobuccal view during surgery. B: photograph of the bone sequestrum after removal. |
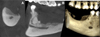 |
Fig. 5 CBCT at the four-month follow-up. A: sagittal view. B: coronal view. C: 3D reconstruction. |
Discussion
This case illustrates the possible occurrence of iatrogenic osteomyelitis following dental extractions in undiagnosed florid cemento-osseous dysplasia. The hypovascular dysplastic bone, characterized by fibrous marrow replacement, impairs perfusion, limits antibiotic diffusion, and delays healing, creating a nidus for chronic infection [5–;7]. Although the infection was primarily attributed to the underlying florid COD, the patient’s comorbidity of type 2 diabetes may have contributed as a minor cofactor by potentially impairing immune response and delaying tissue healing.
Infectious complications occur in approximately 15% of symptomatic COD, with florid forms at highest risk due to multifocality and reduced bone remodeling capacity [4]. Dental extractions are the primary trigger, as demonstrated in a review of 66 infected COD cases [8]. Misinterpretation of COD lesions as periapical pathology often leads to unnecessary interventions, exacerbating risk of iatrogenic complications [5,6].
Radiographically, florid COD presents as a mixed radiolucent–radiopaque lesion with a sclerotic border and a “cotton–wool” appearance. CBCT imaging is essential for accurate diagnosis, lesion mapping, and differentiation from chronic osteomyelitis and ossifying fibroma [3,5,9,10]. Vitality testing of adjacent teeth is critical to avoid misdiagnosis and prevent unnecessary endodontic treatment [7]. Specific diagnostic algorithms have been proposed for suspected COD lesions in the periapical region of endodontically treated teeth.
Management must be conservative. Asymptomatic lesions require only monitoring and oral hygiene reinforcement. When infection occurs, limited surgical debridement and sequestrectomy combined with prolonged antibiotic therapy are considered the treatment of choice [8,11–13]. Similar cases of florid cemento-osseous dysplasia complicated by osteomyelitis have been reported in the literature, emphasizing the role of hypovascular dysplastic bone as a predisposing factor. Most authors describe conservative management combining limited debridement and long-term antibiotic therapy, with favorable outcomes when viable bone is preserved [3,6,7,10,11]. These findings support the therapeutic approach adopted in the present case. Local anesthesia without a vasoconstrictor could theoretically reduce ischemic risk in hypovascular tissue, though evidence is lacking. Successful cases have also been reported with other local anesthetics such as lidocaine/mepivacaine with epinephrine, but no comparative trials exist to guide anesthetic selection [14]. Gentle technique and preservation of viable bone are crucial to reduce recurrence.
Preventive measures are essential to minimize iatrogenic risk. Extractions and implant placement in dysplastic areas should be avoided unless necessary. When unavoidable, atraumatic technique and close postoperative follow-up are mandatory. Prolonged antibiotic therapy until mucosal healing is recommended [6,8]. Long-term radiographic monitoring is essential to detect early relapse or lack of healing [8,11,13].
Implant rehabilitation in COD remains controversial. Some case series report successful osseointegration in stable lesions, but the risk of peri-implant infection remains significant, especially in florid COD [1]. A recent article reported an overall success rate of about 80%, with all failures occurring in florid COD and in implants placed in direct contact with dysplastic bone [15]. These findings confirm that prognosis depends on lesion subtype, vascularity, and implant-to-lesion relationship. A cautious, case-by-case approach is therefore recommended, involving multidisciplinary evaluation and detailed patient consent.
Finally, rare comorbid associations have been described, such as coexistence with bisphosphonate-related osteonecrosis or, exceptionally, osteosarcoma [16,17]. However, a true malignant transformation of COD has never been firmly established, and such cases may represent coincidence rather than causation.
Conclusion
Unwarranted and improperly planned dental extractions in patients with florid cemento-osseous dysplasia can lead to iatrogenic osteomyelitis, as illustrated herein.
Early recognition of COD lesions through pulp vitality testing and CBCT imaging is imperative to prevent unnecessary interventions that can potentially lead to significant iatrogenic complications. Extractions, implants, and endodontic procedures must be strictly avoided in dysplastic areas, unless absolutely necessary.
When osteomyelitis occurs, conservative surgical debridement with sequestrectomy and prolonged antibiotic therapy until mucosal closure is essential for optimal outcomes.
Early identification and preventive management of COD can avert most infectious complications and reduce morbidity. Long-term follow-up is crucial to ensure lesion stability and to detect recurrence or new foci of infection.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare that they have no conflicts of interest in relation to this article.
Data availability statement
No new data were generated or analyzed in support of this research
Ethics approval
Ethical approval was not required.
Informed consent
Informed consent was obtained from the patient.
References
- Hosseinpour S, Khademi MH, Erfani M, Mosaddad SA, Heboyan A. Are implant-based treatments considered viable for patients with focal or florid cemento-osseous dysplasia? A systematic review. Maxillofac Plast Reconstr Surg 2024;46:23. [Google Scholar]
- Wright JM, Vered M. Update from the 4th edition of the World Health Organization classification of head and neck tumours: odontogenic and maxillofacial bone tumors. Head Neck Pathol 2017;11:68–77. [CrossRef] [PubMed] [Google Scholar]
- Cavalcanti PHP, Nascimento EHL, Pontual MLDA, Pontual ADA, Marcelos PGCL de, Perez DE da C, et al. Cemento-Osseous Dysplasias: Imaging Features Based on Cone Beam Computed tomography scans. Braz Dent J 2018;29:99–104. [Google Scholar]
- Decolibus K, Shahrabi-Farahani S, Brar A, Rasner SD, Aguirre SE, Owosho AA. Cemento-osseous dysplasia of the jaw: demographic and clinical analysis of 191 new cases. Dent J (Basel) 2023;11:138. [Google Scholar]
- Daviet-Noual V, Ejeil AL, Gossiome C, Moreau N, Salmon B. Differentiating early stage florid osseous dysplasia from periapical endodontic lesions: a radiological-based diagnostic algorithm. BMC Oral Health 2017;17:161. [Google Scholar]
- Kumar Y, Anand R, Bhagat N, Chakarvarty K, Jaiswal Y. Florid cemento-osseous dysplasia presenting as secondary osteomyelitis: a case report of an undiagnosed condition. Cureus 2024;16:e70291. [Google Scholar]
- Smith MH, Harms PW, Newton DW, Lebar B, Edwards SP, Aronoff DM. Mandibular Actinomyces osteomyelitis complicating florid cemento-osseous dysplasia: case report. BMC Oral Health 2011;11:21. [Google Scholar]
- Kato C de NA de O, de Arruda JAA, Mendes PA, Neiva IM, Abreu LG, Moreno A, et al. Infected cemento-osseous dysplasia: analysis of 66 cases and literature review. Head Neck Pathol 2020;14:173–182. [Google Scholar]
- Alsufyani NA, Lam EWN. Osseous (cemento-osseous) dysplasia of the jaws: clinical and radiographic analysis. J Can Dent Assoc 2011;77:b70. [Google Scholar]
- Singer SR, Mupparapu M, Rinaggio J. Florid cemento-osseous dysplasia and chronic diffuse osteomyelitis report of a simultaneous presentation and review of the literature. J Am Dent Assoc 2005;136:927–931. [Google Scholar]
- Saikia J, Pachipulusu B, Govindaraju P. Florid cemento-osseous dysplasia associated with chronic suppurative osteomyelitis and multiple impacted tooth an incidental finding - a rare case report. J Family Med Prim Care 2020;9:1757–1761. [Google Scholar]
- Demyati AK. Florid cemento-osseous dysplasia associated with secondary infection - a case report. Ann Maxillofac Surg 2023;13:232–235. [Google Scholar]
- Fokam ST, Kwedi GK, Messanga CB. Infected florid cemento-osseous dysplasia: about one clinical observation. Adv Oral Maxillofac Surg 2022;7:100298. [Google Scholar]
- Decani S, Quatrale M, Costa D, Moneghini L, Varoni EM. Florid cemento-osseous dysplasia: a case report and review of literature. Heliyon. 2024;10:e33746. [Google Scholar]
- Hu H, Liu L, Man Y, Ye Z, You M. Clinical and radiologic outcomes of dental implants in cemento-osseous dysplasia: a systematic review and retrospective case series. BMC Oral Health 2025;25:1117. [Google Scholar]
- Indermun S, Titinchi F, Alwan J, Morkel J, Nortje CJ. Osteosarcoma associated with cemento-osseous dysplasia: co-incidence or two related entities? Oral Radiol 2024;40:546–554. [Google Scholar]
- Seo DJ, Moon SY, You JS, Oh JS. Bisphosphonate-related osteonecrosis in a patient with florid cemento-osseous dysplasia. J Oral Med Pain 2024;46:49–46. [Google Scholar]
Cite this article as: Gautier G, Gosseiin-Rousselle L, Henry D, Salmon B, Moreau N. 2026. Iatrogenic osteomyelitis in patients with florid cemento-osseous dysplasia: an illustrative case report. J Oral Med Oral Surg. 32, 2. https://doi.org/10.1051/mbcb/2026005
All Figures
|
Fig. 1 Intraoral view showing swelling and purulent discharge in the right posterior mandible. |
| In the text | |
|
Fig. 2 CBCT scan depicting mixed radiolucent-radiopaque lesions with bone sequestra in the right mandible. A: sagittal view. B: coronal view. C: 3D reconstruction. |
| In the text | |
|
Fig. 3 CBCT panoramic reconstruction illustrating bilateral mandibular involvement with mixed radiolucent and radiopaque areas, typical of florid COD. |
| In the text | |
|
Fig. 4 A: endobuccal view during surgery. B: photograph of the bone sequestrum after removal. |
| In the text | |
|
Fig. 5 CBCT at the four-month follow-up. A: sagittal view. B: coronal view. C: 3D reconstruction. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.