| Issue |
J Oral Med Oral Surg
Volume 31, Number 2, 2025
|
|
|---|---|---|
| Article Number | 18 | |
| Number of page(s) | 7 | |
| DOI | https://doi.org/10.1051/mbcb/2025010 | |
| Published online | 09 June 2025 | |
Original Research Article
Complete-arch implant-supported dental rehabilitations assisted by navigated surgery: a satisfaction study
1
University of Bretagne Occidentale, UFR of Odontology, Brest, France
2
Maxillofacial Surgery, Private Practice, Quimper
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
25
September
2024
Accepted:
12
February
2025
Abstract
Purpose: to evaluate the implant survival and the prevalence of biologic and mechanical complications in edentulous patients restored with implant fixed complete dental prostheses (IFCDPs) assisted by navigated surgery, and to measure the impact on daily life of this prosthetic rehabilitation. Materials and methods: Patients restored with IFCDPs by a single experienced surgeon assisted by the X-Guide navigated surgery tool between 2019 and 2023 were selected. Outcome measures were implant cumulative survival rate (CSR), mechanical prostheses complications and the patient satisfaction was investigated using a standardized questionnaire. Results: A total of 55 patients and IFCDPs were included, totaling 290 implants on 4 mandibles and 51 maxillae. The implant CSR was 100%, no bone loss or implant failure was observed while 8 mechanical complications (15.25%) were reported, including 4 resin losses on TR group and 4 prosthetic tooth fractures in the BED group. Regarding the satisfaction questionnaire, 82% of the patients feeling more comfortable at work and/or in their social life whereas 31% had difficulties pronouncing certain words. Conclusion: This operative procedure assisted by navigated surgery presented reliable clinical outcomes with a high CSR and a high level of patient satisfaction, despite several mechanical complications.
Key words: Complete-arch dental rehabilitation / dental implant / satisfaction study / navigated surgery / all-on-six / implant survival rate / mechanical complications / daily life impactice
© The authors, 2025
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Managing a case of complete rehabilitation in patients with failing dental conditions or complete edentulism is a significant challenge for surgeons. This treatment must aim to restore both aesthetics and function (masticatory comfort). Additionally, it significantly impacts daily life, as complete edentulism is associated with a higher probability of developing depressive syndrome [1] as well as a higher mortality rate [2].
Bone resorption in edentulous patients leads to a modification of anatomical relationships with key anatomical structures, primarily the maxillary sinuses and the inferior alveolar nerves in the mandible.
The advent of navigated surgery in implant dentistry enables more precise three-dimensional implant positioning [3,4] near critical anatomical structures or in areas with limited residual bone quantity. It reduces the need for pre-implant bone graft surgeries and is a preferred alternative to physical surgical guides, which can be restrictive in cases of limited mouth opening and are prone to fracture risks.
Unlike static guided surgery, where a guide is designed and then placed in the mouth to direct drills along a predetermined axis, navigated surgery enables real-time navigation within the patient's bone volume while guided by the implant planification. Using sensors called trackers, the system establishes triangulation between the patient and surgical instruments. This is why navigated surgery has simplified and optimized protocols in implant dentistry as well as in other fields such as spine surgery [5].
Today, implant fixed complete dental prostheses (IFCDPs) are an established approach. A similar retrospective study has reported implant survival rates of 93,3% after 10 years and 87.1% after 20 years [6]. In another study [7], more than 80% of 44 patients rehabilitated by IFCDPs reported being very satisfied regarding the masticatory function and the aesthetics of the prosthesis.
However, this article aims to present the results of a reproducible surgical protocol performed with the assistance of navigated surgery by a single experienced surgeon on a large sample of patients.
Based on the clinical and radiological analysis of 55 cases of complete rehabilitation assisted by navigated surgery provided over a period of 5 years, the primary objective of this study was to analyze the impact that total rehabilitation may have had on the personal and social lives of patients, using a questionnaire given to the patient during the follow-up visit.
The secondary objective was to analyze the reliability and reproducibility of this procedure, analyzing the implant survival rate and the mechanical complications associated with the implant-supported prosthesis.
Materials and methods
In this study, 100 patients who received complete rehabilitation with implant-supported prostheses assisted by the X-Guide navigated surgery tool were selected and contacted. They were operated by the same private practice surgeon between 2019 and 2023. All the patients involved had provided their informed consent prior to inclusion.
This study was approved by the ethical committee of the “Centre Hospitalier de Cornouaille” under approval number 2024-01 for follow-up. The Declaration of Helsinki recognized standards were followed.
The inclusion criteria were as follows:
Clinical and radiological indication for maxillary and/or mandibular complete rehabilitation involving the placement of 4 to 6 angled or non-angled immediate function implants, with loading of a temporary resin bridge within 24 to 48 hours.
Completion of the definitive implant fixed complete dental prostheses by the treating dental surgeon.
At least one implant site requiring guided surgery assistance due to limited bone volume and proximity to critical anatomical structures.
Presence of at least three non-restorable anterior teeth, allowing the attachment of the X-Clip device and calibration of the navigated surgery system.
The exclusion criteria were as follows: cases with incomplete rehabilitation of the arch (preservable teeth or existing implants), absence of navigated surgery during the surgical procedure or presence of a temporary resin bridge.
The surgical protocol was as follows:
• Pre-operative analysis:
Clinical: assessment of non-restorable remaining teeth, analysis of the smile line and Vertical Dimension of Occlusion (VDO) to determine the need for bone resection and the potential provision of a prosthetic false gingiva.
Radiological: planning for the placement of 4 to 6 implants based on available bone volume, angulation of posterior implants at approximately 30° to avoid critical anatomical structures (maxillary sinus, mental nerve loop) using navigated surgery (Fig. 1)
• Surgery:
Posterior implant placement: angled posterior implants were positioned using navigated surgery to avoid anatomical risks (maxillary sinus, mandibular mental nerve loop) using minimally invasive techniques such as flapless surgery or immediate placement in tooth sockets (Fig. 2).
• Anterior implant placement (Fig. 3):
Verification of implant axes: using a hollowed-out guide prosthesis, made from the prosthetic project.
Control of implant placements via retro-alveolar X-rays.
Prosthetic stages: after tightening the multi-unit abutments and radiographic check, an open-tray impression was made using the guide prosthesis and polyether (Impregum®)
Delayed loading: provisional prosthesis placement and occlusal adjustment within 24–48 hours.
At 5 months, the temporary prosthesis was removed and the implant osteointegration was controlled prior to the placement of the definitive prosthesis by the treating dentist.
Inclusion evaluation occured during a follow-up clinic visit, which could take place shortly after loading the provisional bridge or later following placement of the definitive bridge.
Regarding the primary objective, a satisfaction questionnaire (see appendix 1) with 10 binary answer questions (yes/no) was administered to patients during the follow-up visit. This questionnaire assesses the impact of total rehabilitation on masticatory comfort and quality of life.
Regarding the secondary objective, a clinical and radiological examination was performed during the follow-up visit. Potential infectious symptoms were reported and comparison of panoramic radiographs taken previously with those taken on the day of inclusion allowed the assessment of potential bone or implant loss. Mechanical complications, such as fractured teeth on the provisional or definitive prosthesis, were identified during the clinical examination or patient interviews.
The removal of bridges was not performed to probe the implants since this was done annually by the treating dentist who fabricated the final bridge.
Additionally, details regarding the type of definitive restoration performed by the treating dentist (bridge with dental emergence, bridge with false gingiva) and the material used (ceramic, zirconia, resin) were recorded. Furthermore, patients were queried about their comfort levels with the provisional and definitive appliances, including factors such as access to hygiene maneuvers, masticatory comfort and aesthetics.
This study is in compliance with the STROBE checklist.
 |
Fig. 1 Digital planning for the placement of 6 maxillary implants. Note the angulation of the two posterior implants to avoid the maxillary sinus. |
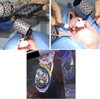 |
Fig. 2 Positioning of posterior angled implant placement using navigated surgery to avoid anatomical risks. |
 |
Fig. 3 Verification of implant axes. |
Results
Between 2019 and 2023, 55 of the 100 selected patients were included during the follow-up visits. Among them, there were 29 women and 26 men aged between 43 and 90 years at the time of their procedures, with an average age of 70 years. They received complete maxillary or mandibular rehabilitation with immediate loading of an implant-supported prosthesis facilitated by the navigated surgery system X-Guide®.
Out of the 100 selected patients, 33 patients did not respond to the invitations or were unable to attend the clinic. Twelve patients were excluded from the study during the follow-up because they did not meet the inclusion criteria: 5 of them whose intervention ultimately did not require the use of the navigated surgery, 5 who still had their provisional prostheses in polymethyl methacrylate (PMMA) resin and 2 who presented a fully fixed removable prosthesis.
Inclusion periods extended from November 2023 to February 2024. Thirteen patients were operated in 2019, 2 in 2020, 16 in 2021, 13 in 2022, and 11 in 2023.
Thirty-five complete rehabilitations with 6 implants (All-On-6) and 20 complete rehabilitations with 4 implants (All-On-4) were performed with the assistance of navigated surgery, totaling 290 implants on 4 mandibles and 51 maxillae.
Regarding the type of rehabilitation, 55 definitive complete prostheses were recorded, including 39 bridges with a titanium framework, prosthetic gum made of resin and ceramic teeth (Titanium Resin TR) (Fig. 4) and 16 zirconia-based Bridges with Dental Emergence (BED) (Fig. 5) (12 zirconia-ceramic, 4 monolithic zirconia).
Regarding the primary objective, the questionnaire reflected the impact of fixed full arch rehabilitation on the 55 included patients, with 89% of them experiencing an improvement in self-image and 82% feeling more comfortable at work and/or in their social life, mainly due to improved comfort during eating (87%). Approximately 69% had difficulties pronouncing certain words. As for the question “Would you undergo this intervention again if given the choice?”, 89% of patients answered positively. (Tabs. I and II).
Regarding the secondary objective, the Cumulative Survival Rate (CSR) was 100%. No implant failure was observed among the 290 implants placed between 2019 and 2023. No bone or implant loss was observed on panoramic radiographs (Fig. 6). Additionally, no infectious symptoms were reported by the patients.
During the interviews and clinical examinations, 8 mechanical complications were reported among 55 appliances, representing a 14,55% complication rate : 1 in a patient who underwent surgery in 2019, 4 in 2021 while 3 appeared in patients who underwent surgery/operated after 2022.
Regarding BED, there was a 25% complication rate with 4 prosthetic tooth fractures observed, including 3 in ceramic (chipping) and 1 in monolithic zirconia (Fig. 7). As for TR, 4 instances of resin loss on titanium and resin bridges with prosthetic gums were reported, representing 10.26% (Tab. III).
 |
Fig. 4 Bridge with a titanium framework, false gingiva made of resin and ceramic teeth. |
 |
Fig. 5 Zirconia-based bridge with dental emergence. |
Summary of results obtained from the binary questionnaire.
Satisfaction rate.
 |
Fig. 6 Panoramic radiograph showing no bone loss around implants. |
 |
Fig. 7 Prosthetic tooth fracture observed on a monolithic zirconia bridge. |
Mecanical complications − Survival Curve.
Discussion
Regarding the satisfaction study, the questionnaire revealed another complication: speech difficulties. Notably, 31% of patients had trouble pronouncing some words. This can be explained by several factors: adaptation to a new proprioception, gingival retraction after healing (which can create a space between the mucosa and the inner surface of the bridge) and a change in tooth length. This complication most often occurs during the placement of the provisional bridge and disappears when the dentist makes the final denture, which is more adapted to the mucosa. Only 21% of patients reported changing their eating habits.
In terms of comfort, 87% of patients felt more comfortable with their diet, and 89% were satisfied with the aesthetics and self-image. Similar rates were found in the study by Tang et al. [7], where over 80% of 30 patients were “very satisfied” with masticatory comfort and the aesthetics of their complete rehabilitation, but 13.6% were not satisfied with word pronunciation since the placement. A study on hybrid complete rehabilitations with two zygomatic posterior implants [8] found 89% satisfaction for masticatory comfort, 94% satisfaction with aesthetics, but 27% were ambivalent or dissatisfied with speech.
The implant survival rate was 100% out of 290 implants, based on panoramic X-Ray and clinical exam. This rate is similar to data found in the literature: two retrospective studies over 5 years involving 44 and 43 implant fixed complete dental protheses (IFCDPs) reported survival rates of [92.5%–99.3%] [7] and 100% [9] respectively.
Mechanical complications represented approximately 15% of the 55 IFCDPs, with 25% for BED and 10% for TR, a low rate compared to another similar study [7] which found 65.9% (29 out of 44 prostheses; 45.5% ceramic chipping; 13.6% crown dislodgment; 4.5% framework fracture; 2.3% crown fracture), with no significant difference between TR and BED groups. One-quarter (4 out of 16) of BED IFCDPs experienced a mechanical issue. Another study [10] involving 92 ceramic-veneered zirconia frameworks BED estimated the 5-year risk of any mechanical complication to be 90.5%, primarily due to ceramic chipping.
In this study, only 4 mandibles were operated on compared to 51 maxillae. Indeed, navigated surgery is particularly beneficial for angled posterior maxillary implants as it helps avoid flap elevation to locate the sinus.
This retrospective study with a follow-up period of up to 5 years has several limitations. A study with a more extensive follow-up and a larger sample size is necessary to confirm the long-term viability of this operative protocol. Additionally, IFCDPs were not removed, which did not allow the analysis of biologic complications.
Conclusion
This complete-arch implant-supported dental rehabilitation assisted by navigated surgery demonstrated excellent clinical outcomes with a high level of patient satisfaction and a high implant survival rate over a follow-up period of up to 5 years for 55 patients, despite several mechanical complicationsBas du formulaire. Considering the limitations of this retrospective study, this procedure appears reliable and reproducible if the navigated surgical tool is well mastered. It simplifies treatment plans and offers a certain level of comfort to patients by avoiding pre-implant bone grafts through navigated surgery and angled posterior implants.
Acknowledgments
Thanks to Sylvie Boisramé who, as thesis director, allowed me to better organize my ideas and finalize this article. Thanks to Julien Guiol whose clinical and surgical perspective enabled this study.
Funding
This research did not receive any specific funding.
Conflicts of interest
There are no conflicts of interest to declare.
Data availability statement
The data supporting the findings of this study are openly available.
Author contribution statement
J.D. and J.G. conceived the ideas, collected and analysed the data. JD. and S.B. led the writing.
References
- Tyrovolas S, Koyanagi A, Panagiotakos DB, Haro JM, Kassebaum NJ, Chrepa V, et al. Population prevalence of edentulism and its association with depression and self-rated health. Sci Rep. 2016;6: 37083. [CrossRef] [Google Scholar]
- Brown DW. Complete edentulism prior to the age of 65 years is associated with all‐cause mortality. J Public Health Dent 2009;69: 260–266. [CrossRef] [PubMed] [Google Scholar]
- Wei SM, Zhu Y, Wei JX, Zhang CN, Shi JY, Lai HC. Accuracy of dynamic navigation in implant surgery: a systematic review and meta-analysis. Clin Oral Implants Res 2021;32: 383–393. [CrossRef] [PubMed] [Google Scholar]
- Stefanelli L, DeGroot B, Lipton D, Mandelaris G. Accuracy of a dynamic dental implant navigation system in a private practice. Int J Oral Maxillofac Implants 2019;34: 205–213. [CrossRef] [PubMed] [Google Scholar]
- Rawicki N, Dowdell JE, Sandhu HS. Current state of navigation in spine surgery. Ann Transl Med 2021;9: 85. [CrossRef] [PubMed] [Google Scholar]
- Chrcanovic BR, Kisch J, Larsson C. Retrospective evaluation of implant‐supported full‐arch fixed dental prostheses after a mean follow‐up of 10 years. Clin Oral Implants Res 2020;31: 634–645. [CrossRef] [PubMed] [Google Scholar]
- Tang Y, Yu H, Wang J, Qiu L. Implant survival and complication prevalence in complete-arch implant-supported fixed dental prostheses: a retrospective study with a mean follow-up of 5 years. Int J Oral Maxillofac Implants 2023;38: 84–93. [CrossRef] [PubMed] [Google Scholar]
- Pesce P, Menini M, Bagnasco F, Gamalero M, Pera F, Tealdo T. Outcomes of Zygomatic implants combined with anterior regular implants: a retrospective analysis with a mean follow-up time of 36 months. Int J Oral Maxillofac Implants 2023;38: 251–258. [CrossRef] [PubMed] [Google Scholar]
- Caramês J, Duarte Sola Pereira Da Mata A, Nuno Da Silva Marques D, Francisco H. Ceramic-veneered zirconia frameworks in full-arch implant rehabilitations: a 6-month to 5-year retrospective cohort study. Int J Oral Maxillofac Implants 2016;31: 1407–1414. [CrossRef] [PubMed] [Google Scholar]
- Chochlidakis K, Ercoli C, Einarsdottir E, Romeo D, Papaspyridakos P, Barmak AB, et al. Implant survival and biologic complications of implant fixed complete dental prostheses: an up to 5-year retrospective study. J Prosthet Dent 2022 128:375–381. [CrossRef] [PubMed] [Google Scholar]
Cite this article as: Douley J, Boisramé S, Guiol J, 2025. Complete-arch implant-supported dental rehabilitations assisted by navigated surgery: a satisfaction study. J Oral Med Oral Surg. 31, 18: https://doi.org/10.1051/mbcb/2025010
All Tables
All Figures
|
Fig. 1 Digital planning for the placement of 6 maxillary implants. Note the angulation of the two posterior implants to avoid the maxillary sinus. |
| In the text | |
|
Fig. 2 Positioning of posterior angled implant placement using navigated surgery to avoid anatomical risks. |
| In the text | |
|
Fig. 3 Verification of implant axes. |
| In the text | |
|
Fig. 4 Bridge with a titanium framework, false gingiva made of resin and ceramic teeth. |
| In the text | |
|
Fig. 5 Zirconia-based bridge with dental emergence. |
| In the text | |
|
Fig. 6 Panoramic radiograph showing no bone loss around implants. |
| In the text | |
|
Fig. 7 Prosthetic tooth fracture observed on a monolithic zirconia bridge. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.