| Issue |
J Oral Med Oral Surg
Volume 30, Number 2, 2024
|
|
|---|---|---|
| Article Number | 15 | |
| Number of page(s) | 7 | |
| DOI | https://doi.org/10.1051/mbcb/2024018 | |
| Published online | 08 August 2024 | |
Original Research Article
Evaluation of early marginal bone loss around posterior dental implants placed in axial and non-axial positions: a retrospective cone beam computed tomography (CBCT) analysis
Department of Periodontics and Implantology, Vishnu Dental College, Vishnupur, Bhimavaram 534202, West Godavari, Andhra Pradesh, India
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
11
November
2023
Accepted:
20
June
2024
Abstract
Introduction: To retrospectively assess the mesio-distal angular deviation/inclination of single implants restored in the posterior edentulous arches and evaluate the effect of angular deviations on the early bone loss after 12 months of functional implant loading. Materials and methods: This retrospective Cone beam computed tomography (CBCT) analysis assessed 60 single implants including 36 axially placed (AX Group) and 24 non-axially (NAX Group) placed implants of dimension 4.2 × 10 mm. Marginal bone loss (Mesial, Distal) was assessed at 1 year post implant loading in both maxillary and mandibular implants. Independent sample t-test was done for intergroup comparison and paired t-test for intragroup comparisons. Results: Mean MBL was significantly greater (P-0.02) in NAX group compared to AX group on both mesial and distal sides. Maxillary implants showed greater MBL (3.17 ± 1.33, 2.99 ± 1.63 on mesial and distal sides respectively) compared to mandibular implants (1.86 ± 0.53, 2.29 ± 0.90 on mesial and distal sides respectively). Conclusion: Greater mean MBL during first year of functional loading in NAX group and maxillary implants was observed with minimal post-operative complications and good survival rate in both groups.
Key words: Bone loss / cone beam computed tomography / dental implant loading / dental implant single tooth
© The authors, 2024
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Dental implants have emerged as one of the successful treatment modalities for replacement of missing teeth. Success of implant treatment depends on various aspects [1,2], the angle at which the implant is placed is one such [3]. Various conditions such as available bone, ridge resorption, bony protuberances, anatomical sites, implant size and length etc., will determine the angle (non-axially) at which the implant must be placed [4]. Regenerative procedures such as sinus augmentation, guided bone regeneration, block grafting and alternative techniques such as pterygoid, tuberosity, zygomatic and short implants provide an alternative for inadequate available bone [5–9]. However, these procedures require clinical expertise and often pose surgical and post-operative risks and complications along with delayed treatment time. Hence non-axial implant placement has been practiced as a viable treatment option [10–12].
Due to the absence of the periodontal ligament, dental implants are less resilient to traumatic occlusal forces than natural teeth. Hence, dental implants are more vulnerable to increased torsional and shear stresses harming the bone to implant contact acting on the surrounding bone due to non-axial forces [13]. Non-axial implant angulation is often thought to be one common reason for implant failure due to transfer of abnormal forces to the surrounding bone and leading to crestal bone resorption and peri-implantitis [14]. However, tilting implants in non-axial position still remains a controversy with variable outcomes ranging from similar clinical effectiveness to increased peri-implant bone loss/failure of non-axial implants [15–17].
Therefore, the aim of the current research was to find the association between angle of the implants and marginal bone loss in axial and non-axial implants using cone beam computed tomographic images (CBCT) taken at baseline and 1 year after functional loading.
Materials and Methods
Study protocol and data collection
The Institutional Ethical Committee accepted this study protocol, which followed the 2013 Helsinki Declaration. This is a retrospective CBCT analysis in which CBCT data from 78 participants who underwent single posterior implant (4.2 × 10mm) placement between March 2020 to April 2021 were collected and evaluated for possible inclusion in the study.
Sample size
After final evaluation of the data and exclusion of subjects this retrospective CBCT analysis assessed 54 participants who received 60 implant supported restorations between March 2020 and April 2021 based on convenience sampling. 36 implants were placed in axial (AX) and 24 implants in non-axial (NAX) inclinations in the posterior edentulous sites. Implants of size 4.2 × 10 mm with delayed loading protocol (implants loaded 3–4 months after implant placement) in all the participants were evaluated at least 12 months after loading. Marginal bone level i.e., mesial and distal was evaluated at 12 months after loading.
Selection criteria
The images chosen for this study had to meet the following inclusion criteria: (a) the presence of opposing maxillary/mandibular teeth to provide information for implant location and angulation; (b) the presence of healthy periodontium on adjacent teeth with no signs of bone loss radiographically; (c) the absence of peri-implant mucositis/peri-implantitis in the past; (d) presence of opposing natural teeth and (e) maintaining good oral hygiene with full mouth bleeding and plaque scores of 15%. The percentage of tooth surfaces that showed the presence of plaque detected by using a periodontal probe was calculated to determine the full mouth plaque score (FMPS) [18]. The full mouth bleeding score (FMBS), was based on the presence or absence of bleeding up to 30 seconds after probing. The exclusion criteria were a; incomplete medical records, b; presence of systemic diseases and conditions, c; pregnant or lactating women, d; immuno-deficiency disorders, e; patients who underwent radiotherapy in the head and neck regions, f; history of smoking/alcohol consumption, g; presence of periapical radiolucency's on adjacent teeth, h; unclear images because of scattering or beam-hardening artifacts, i; implants placed in sites treated with bone augmentation, j; unerupted or incompletely erupted teeth adjacent to implant site, k; parafunctional habits. The demographic, clinical and radiographic data of all the participants were obtained from electronic medical record management system.
CBCT image analysis and assessment
The three-dimensional (3D) images of implants in the maxillary and mandibular premolar and molar region were reconstructed using 3D visualization and were evaluated by using SCANORA™ Imaging software 5.2 version (ON DEMAND 3D™ server Tuusula, Finland). Cranex 3D (Sordex, Tuusula, Finland) at 90 kVp and 8 mA with an exposure length of 10 seconds was used to get a good quality image of posterior sextants. The pictures had 0.13 mm voxels, a field of view of 6 × 4 cm, and a slice thickness of 0.25 mm.
CBCTs of 78 participants were assessed out of which 60 CBCT's of 54 participants fulfilling all the selection criteria were included. CBCTs of 18 participants were excluded, the main reasons being presence of unerupted adjacent teeth, unclear CBCT images and lack of 12 months post loading CBCT images. Based on the availability of CBCT images during the study period i.e., March 2020 to April 2021 the CBCT images were categorized into axial (AX) and Non-axial (NAX) groups (Fig. 1).
 |
Fig. 1 Patient allocation flow chart. |
Outcome assessment
The primary outcome was the assessment of marginal bone level (MBL) in relation to implant inclination i.e., AX or NAX. MBL was described as level of alveolar bone that is marginally adjacent to a dental implant in an apical position. The marginal bone loss was described as the relative change in the position of marginal bone at 12 months after functional loading from the marginal bone level during functional loading. Prior to the start of the study CBCT analysis was done for 5 CBCT images by a single examiner at three different intervals. A reproducibility of <1 mm for marginal bone loss for 95% of recordings was considered acceptable. Intra-examiner correlation coefficient (k = 0.87) was considered reliable. By comparing CBCT images taken immediately following prosthesis delivery with those taken one year after functional loading (i.e., at-least 3 months after implant placement), the peri-implant marginal bone-level change was calculated. When determining the level of marginal bone, the fixture's intersection of the polished and rough surfaces is used as a reference point. By calculating the distance between the reference point and the most apical point of the bone level, marginal bone levels at the mesial and distal implant surfaces were evaluated in cross-sectional view. The implant inclination was classified as AX with an inclination between 0 and 10 degrees and NAX with an inclination between 11 and 30 degrees. It was defined as the angle between the implant's long axis and the occlusal plane [17] (Fig. 2).
Statistical analysis
SPSS (version 15.0, IBM, Chicago, IL) software was used for statistical analysis of the data collected. Paired t-test was used for the intra-group comparison. Using an independent sample t test, intergroup comparisons were made. The data were presented using the odds ratio (OR) and a 95% confidence interval. p-value < 0.05 was considered as statistically significant.
Results
A total of 60 CBCT images of 54 clinical patients, with 48 patients who received single implants and 6 patients received non adjacent two implants. A total of 24 males and 30 females were selected. The patients' ages ranged from 31 years to 56 years, and their mean age was 42.4 ± 13.2 years. No signs of post-operative complications were reported and the healing was uneventful in both groups. A survival rate of 100% was observed in both groups.
Intragroup comparison of MBL from baseline to 12 months post loading showed highly significant (P < 0.001) increase in MBL in both groups. Mean MBL on mesial side was significantly greater (p = 0.02) in NAX group (3.17 ± 1.65mm) compared to AX group (2.14 ± 0.60 mm) (Tab. I). Similarly, mean MBL on distal side was also significantly greater in NAX group compared to AX group (p = 0.02) (Tab. II and Fig. 2).
Intragroup comparison of MBL in AX group between maxillary and mandibular implants showed significant increase (p = 0.001) from baseline to 12 months with maxillary implants (3.17 ± 1.33, 2.99 ± 1.63 on mesial and distal side respectively) showing greater MBL compared to mandibular implants (1.86 ± 0.53, 2.29 ± 0.90 on mesial and distal sides respectively) (Figs. 2 and 3).
NAX group also showed significant increase in MBL from baseline to 12 months in both maxillary (2.71 ±.77, 3.04 ± 0.84 on mesial and distal sides) and mandibular (2.42 ± 0.80, 2.76 ± 1.03 mm on mesial and distal sides) implants. However, intergroup comparisons showed only significant difference (p = 0.03) in the mean MBL between maxillary and mandibular implants on mesial side in NAX group (Tab. III, Figs. 4 and 5).
Marginal bone level (MBL) in non-axial (NAX) and axial (AX) implants.
Marginal bone level (MBL) in maxillary vs. mandibular implants in AX group.
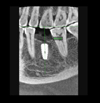 |
Fig. 2 Assessment of Mesio-Distal implant inclination i.e., angle between the implant's long axis and the occlusal plane at baseline in axial implants. |
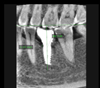 |
Fig. 3 Assessment of peri-implant marginal bone level at 12 months implant functional loading in axial group. |
Marginal bone level (MBL) in maxillary vs. mandibular implants in NAX group.
 |
Fig. 4 Assessment of peri-implant marginal bone level at baseline in non-axial group. |
 |
Fig. 5 Assessment of peri-implant marginal bone level at 12 months implant functional loading in non-axial group. |
Discussion
In the present study the incidence of marginal bone loss (MBL) around single implants placed in axial (AX) and non-axial (NAX) inclinations was assessed at 12–15 months after functional loading. The results of this study demonstrated that significant correlation exists between the implant inclination and crestal bone loss over the 1-year of functional loading of single implants placed in the posterior region. The mean MBL was significantly greater in NAX group compared to AX group (p = 0.02). Similar study by Koutouzis et al. in 2007 retrospectively analyzed the potential influence of implant inclination on marginal bone loss at freestanding, implant-supported, fixed partial dentures (FPDs) over a 5-year period of functional loading and reported no significant difference (P > 0.05) in the mean marginal bone loss between axial (0.4 mm) and non-axial (0.5 mm) implants [17]. However, the above study by Koutouzis et al. assessed marginal bone loss at implants supported fixed partial denture. Till date no clinical study assessed the marginal bone loss around single implants in relation to implant inclination/angulation. In longitudinal studies that evaluate implant therapy, assessment of marginal/crestal bone loss surrounding implants is frequently utilized as a primary outcome measure. After the first year of function, early crestal bone loss is frequently seen, followed by minor bone loss (0.2 mm) annually [19]. Despite the fact that many other factors are addressed, occlusal stress and inflammation brought on by biofilm production are frequently regarded as having the most effects on the peri-implant marginal bone-level change [20].
Dong-Won Lee in 2014 evaluated the impact of single dental implants placed in the first molar region off-axially in terms of the impact of the crown width-fixture width ratio on crestal bone loss. He found that after one year of functional loading, off-axial loading caused by a high crown width-fixture width ratio did not increase the risk for peri-implant marginal bone loss [21]. In contrast to this study, Kim et al. (2011) assessed photo elastically the impact of the All-on-Four concept's tilt of the two distal implants on the distribution of stress inside the supporting framework. They reported that, compared to axial implants, the use of tilted implants lowered the maximum stress in the distal crestal bone of the distal implant by about 17% [22].
Osseo-integrated implants, unlike natural teeth, are ankylosed to surrounding bone without the periodontal ligament, which has mechanoreceptors and serves as a shock absorber. Additionally, it has been suggested that dental implants may be more vulnerable to crestal bone loss caused by mechanical stress since the crestal bone around them may act as a pivot point for a lever action when a bending moment is applied. Prostheses supported by 1 or 2 implants in the posterior region, straight implant alignment, significant deviation of the implant axis from the line of action, high crown/implant ratio, excessive cantilever length, discrepancy in dimensions between the occlusal table and implant head, and parafunctional habits are all contributing factors associated with increased bending overload in dental implants. The marginal bone level may be negatively impacted by excessive stress on the surrounding bone that supports the implant. Shear force is known to be least resistive to the cortical bone, and bending overload considerably increases this resistance.
The current research however reported no signs of severe post loading complications such as implant/Screw/prosthesis fractures or failure of implants in both groups except for screw loosening and crown dislodgement observed in 4 cases of non-axial implant position with 100% survival rate and a mean marginal bone loss of 1.5 mm in AX group and 2.0 mm in NAX group. A retrospective research on the surgical results of angulated/ tilted implants i.e., with implant mesio-distal angulation of >15° in severely resorbed edentulous maxilla as an alternative to bone grafting was conducted by Rosen and Gynther. With a mean bone loss of 1.2 mm during the first year of functional loading, they observed a 97% success rate in 19 patients with long-term follow-up of almost 10 years [5]. Inclination of implants can cause a severe mis-angulation (>25 degrees) or a minor mis-angulation (0–15 degrees). Minor mis-angulations of <15 degrees is easy to manage by use of prefabricated custom crowns. However, major mis-angulations of greater than 15 degrees require fabrication of custom angulated abutments and require extra space to hold the implant supported crown.
To support fixed prosthesis in an atrophic maxillary arch, Almeida et al. used a finite element analysis (FEA) model to compare the biomechanical behavior of tilted long implant and vertical short implant. They found that the presence of distal tilted (all-on-four) and distal short implants (all-on-six) resulted in higher stresses in both situations compared to the presence of vertical implants (all-on-four) [8]. Additionally, because to the high forces put on the implant-abutment contact, it is possible for an implant's coronal portion to fracture, a screw to break, or an abutment screw to loosen. The higher masticatory forces will make these difficulties exacerbated in the posterior region.
The current study is a retrospective observational study with few limitations such as a short term follow up of 12 months as well as inclusion of single missing posterior teeth. Therefore, the results cannot be generalized to all the clinical scenarios. Long term assessment considering different clinical conditions such as full mouth rehabilitation and implant supported fixed prosthesis using angulated may provide a better understanding.
Conclusion
Greater mean marginal bone loss was observed in non-axial implant position especially in maxillary implants compared to axial and mandibular implants with no early prosthetic complications in either of the groups.
Funding
There is no source of funding or grant from any of the organization or institute or individual towards this study.
Conflicts of interest
The other authors do not have any financial interests, either directly or indirectly, in the products or information listed in the paper.
Data availability statement
All the data related to the current research is available in the manuscript. No additional information is required to be available in other sources.
Ethics approval
The study was approved, and ethical clearance was obtained from the Institutional ethical committee with Ref. No.: IECVDC/2021/PG01/PI/IVV/18.
Informed consent
Before the start of research the study design was explained to all the participants and written informed consent was obtained from all the participants.
Permission to reproduce material from other sources
All the data provided in the article is original and not from any other sources.
References
- Raikar S, Talukdar P, Kumari S, Panda SK, Oommen VM, Prasad A. Factors affecting the survival rate of dental implants: a retrospective study. J Int Soc Prev Commun Dent 2017;7:351–355. [CrossRef] [PubMed] [Google Scholar]
- Yang Y, Hu H, Zeng M, Chu H, Gan Z, Duan J et al. The survival rates and risk factors of implants in the early stage: a retrospective study. BMC Oral Health. 2021;21:293. [CrossRef] [Google Scholar]
- Wright SP, Hayden J, Lynd JA, Walker-Finch K, Willett J, Ucer C, Speechley SD. Factors affecting the complexity of dental implant restoration − what is the current evidence and guidance? Br Dent J 2016; 18;221(10): 615–622. [CrossRef] [PubMed] [Google Scholar]
- Mehta SP, Sutariya PV, Pathan MR, Upadhyay HH, Patel SR, Kantharia ND. Clinical success between tilted and axial implants in edentulous maxilla: a systematic review and meta-analysis. J Indian Prosthodontic Soc 2021;21:217. [CrossRef] [PubMed] [Google Scholar]
- Rosen A, Gynther G. Implant treatment without bone grafting in edentulous severely resorbed maxillas: a long-term follow-up study. J Maxillofac Surg 2007;65:1010–1016. [CrossRef] [Google Scholar]
- Patel K, Madan S, Mehta D, Shah SP, Trivedi V, Seta H. Basal implants: an asset for rehabilitation of atrophied resorbed maxillary and mandibular jaw − a prospective study. Ann Maxillofac Surg 2021;11:64–69. [Google Scholar]
- Manacorda M, Poletti de Chaurand B, Merlone A, Tetè G, Mottola F, Vinci R. Virtual implant rehabilitation of the severely atrophic maxilla: a radiographic study. Dent J (Basel). 2020;8:14. [Google Scholar]
- Almeida EO, Rocha EP, Freitas Júnior AC, Anchieta RB, Poveda R, Gupta N, Coelho PG. Tilted and short implants supporting fixed prosthesis in an atrophic maxilla: A 3D-FEA biomechanical evaluation. Clin Implant Dent Related Res 2015; 17 Suppl 1: e332–e 342. [Google Scholar]
- Abdel-Khalek EA, Khalifa AK, Elmekawy N. The effect of using prefabricated bars on marginal bone loss around tilted or axially placed and immediately loaded implants for retaining mandibular overdentures. J Dent Implant 2018;8:54. [CrossRef] [Google Scholar]
- Malo P, Miguel de Araujo N, Lopes A. Preliminary report on the outcome of tilted implants with longer lengths (20-25 mm) in low-density bone: one-year follow up of a prospective cohort study. Clin Implant Dent Related Res 2013;17:134–142. [Google Scholar]
- Nag PVR, Sarika P, Khan R, Bhagwatkar T. Tall and tilted pin hole immediately loaded implants (TTPHIL) technique for maxillary arch rehabilitation. Int J Res Rev 2018;5:104–110. [Google Scholar]
- Nag PVR, Sarika P, Bhagwatkar T, Dhara V. Pterygoid implant: option for rehabilitation of the atrophic posterior maxilla. Int J Contemp Dent Med Rev 2019;19:1–6. [Google Scholar]
- Rodrigues VA, Tribst JPM, de Santis LR, de Lima DR, Nishioka RS. Influence of angulation and vertical misfit in the evaluation of micro-deformations around implants. Braz Dent Sci 2017;20:32–39. [CrossRef] [Google Scholar]
- Rodrigues VA, Tribst JPM, Santis LR, Borges ALS, Nishioka RS. 2018. Biomechanical effect of inclined implants in fixed prosthesis: strain and stress analysis. Rev Odontolog UNESP 47:237–243. [CrossRef] [Google Scholar]
- Rangert B, Krogh PH, Langer B, Van Roekel N. Bending overload and implant fracture: a retrospective clinical analysis. Int J Oral Maxillofac Implants 1995;10:326–334. [PubMed] [Google Scholar]
- Vasconcellos LG, Nishioka RS, Vasconcellos LM, Balducci I, Kojima AN. Microstrain around dental implants supporting fixed partial prostheses under axial and nonaxial loading conditions, in vitro strain gauge analysis. J Craniofac Surg 2013;24:e54651. [CrossRef] [PubMed] [Google Scholar]
- Koutouzis T, Wennström JL. Bone level changes at axial- and non-axial-positioned partial implants supporting fixed dentures. A 5-year retrospective longitudinal study. Clin Oral Implants Res 2007;18 (5): 585–590. [CrossRef] [PubMed] [Google Scholar]
- O'Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol 1972;43:38. [CrossRef] [PubMed] [Google Scholar]
- Pérez-Pevida E, Chávarri-Prado D, Diéguez-Pereira M, Estrada-Martínez A, Montalbán-Vadillo O, Jiménez-Garrudo A. Consequences of peri-implant bone loss in the occlusal load transfer to the supporting bone in terms of magnitude of stress, strain, and stress distribution: a finite element analysis. Biomed Res Int. 2021;2021:3087071. [Google Scholar]
- Lee DW, Lee DW, Park KH, Moon IS. The effects of off-axial loading on periimplant marginal bone loss in a single implant. J Prosthet Dent 2014;112:501–507. [CrossRef] [PubMed] [Google Scholar]
- Kim KS, Kim YL, Bae JM, Cho HW. Biomechanical comparison of axial and tilted implants for mandibular full-arch fixed prostheses. Int J Oral Maxillofac Implants 2011;26: 976–984. [PubMed] [Google Scholar]
- Oh TJ, Yoon J, Misch CE, Wang HL. The causes of early implant bone loss: myth or science? J Periodontol 2002;73:322–333. [CrossRef] [PubMed] [Google Scholar]
All Tables
All Figures
|
Fig. 1 Patient allocation flow chart. |
| In the text | |
|
Fig. 2 Assessment of Mesio-Distal implant inclination i.e., angle between the implant's long axis and the occlusal plane at baseline in axial implants. |
| In the text | |
|
Fig. 3 Assessment of peri-implant marginal bone level at 12 months implant functional loading in axial group. |
| In the text | |
|
Fig. 4 Assessment of peri-implant marginal bone level at baseline in non-axial group. |
| In the text | |
|
Fig. 5 Assessment of peri-implant marginal bone level at 12 months implant functional loading in non-axial group. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.