| Issue |
J Oral Med Oral Surg
Volume 25, Number 1, 2019
|
|
|---|---|---|
| Article Number | 7 | |
| Number of page(s) | 2 | |
| Section | Cas clinique / Short case report | |
| DOI | https://doi.org/10.1051/mbcb/2018031 | |
| Published online | 22 February 2019 | |
Short Case Report
Extensive amalgam tattoo (amalgam pigmentation) on the palatal mucosa: a short case report
1
Service de chirurgie maxillo-faciale, Stomatologie et chirurgie plastique. Hôpital militaire d'instruction Mohammed V, Rabat, Morocco
2
Laboratoire d'Anatomopathologie, Hôpital militaire d'instruction Mohammed V, Rabat, Morocco
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
18
January
2018
Accepted:
6
July
2018
Abstract
Introduction: An amalgam tattoo is the most common form of exogenous oral pigmentation caused by the diffusion of dental amalgam into the soft tissue. Observation: Here we describe a case of diffuse pigmentation of amalgam on the hard palate. Discussion: Mucosal hyperpigmentation can occasionally be confused with melanotic lesions, thereby requiring a biopsy for differential diagnosis. Once the diagnosis of an amalgam tattoo has been established, the removal of the lesion is not necessary, except for aesthetic reasons.
Key words: amalgam tattoo / oral mucosa / pigmentation
© The authors, 2019
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Observation
A 56-year-old man with an unremarkable medical history was referred to the department of maxillofacial surgery due to suspected mucosal melanoma. Clinical examination revealed a large, dark, flat macula located on the right hard palate adjacent to tooth 16 which had been restored using amalgam fillings (Fig. 1). There was no lymphadenopathy. Panoramic X-ray examination did not exhibit any abnormalities. Biopsy was then performed under local anesthesia. Histology showed a brownish-black pigment along the collagenous fibers and in the vascular sheaths. No melanocytes or nevus cells were found (Fig. 2). The findings suggested the diagnosis of an amalgam tattoo. The patient needed no further treatment.
 |
Fig. 1 A 56-year old man with a large mucosal pigmentation, extending from the right maxillary canine to the tuberosity. |
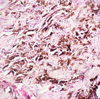 |
Fig. 2 Histological section of the palatal mucosa. |
Discussion
Amalgam tattoos are common, exogenous, pigmented lesions of the oral mucosa, resulting mainly from the accidental displacement of metal particles in oral soft tissues during restorative dental procedures using amalgam. The diagnosis is simple; clinically, amalgam tattoo presents as slate-gray, bluish, or black macules. Lesions are usually uniformly round, uniformly pigmented, and measure between 0.1 and 2 cm [1]. They mainly affect the mandibular gingival mucosa, buccal mucosa, floor of the mouth, tongue, retromolar mandibular area, lips, and palate [2]. Periapical X-ray examination may be useful to detect the radiopacity associated with amalgam. However, less than 25% of amalgam pigmentations are radiopaque and visible on radiography [2,3].
An amalgam tattoo may require biopsy when it is mis diagnosed as melanosis (especially when there is no radiopacity) or located near any restored teeth. In the present case, biopsy was performed due to the large size of the lesion. Microscopic examination reveals an intact surface epithelium and a fine golden-brown granule, which can be found along connective tissues and is basically a staining membrane of golden-brown color (this may be the only sign of an amalgam tattoo); dense fibrosis and scarring are usually present, and a granulomatous reaction may be associated [4]. The diagnosis of an amalgam tattoo can be difficult to discern from other pigmented elements of the oral mucosa, including mucosal melanoma, nevocellular nevus and blue nevus, hemangioma, postinflammatory pigmentation, smoker's melanosis, drug-induced hyperpigmentation, and oral pigmentation associated with systemic diseases (e.g., Addison's disease, Albright's syndrome, acromegaly, and Nelson's syndrome) [5]. The removal of the amalgam is not necessary, except for cosmetic reasons. If the pigmentation is cosmetically unacceptable, surgical excision and transplantation of the oral mucosal tissue can be performed. Q-switched ruby laser and Q-switched alexandrite laser have been used with favorable results [4]. In the present case, there was no need to remove the pigmentation because it did not cause any esthetic or functional discomfort to the patient.
Conclusion
An amalgam tattoo is one of the most common causes of exogenous pigmentation in the oral mucosa. The reported case showed an unusual form of an extensive amalgam tattoo, probably due to the continual migration of metal particles to the palatal mucosa during chewing. The therapy most often involves surgical excision, but recently, laser therapy has provided exceptional results.
Conflicts of interest
The authors declare that they have no conflicts of interest in relation to this article.
References
- Meleti M, Vescovi P, Mooi WJ, Van der Waal L. Pigmented lesions of the oral mucosa and perioral tissues: a flow-chart for the diagnosis and some recommendations for the management. Oral Surg Oral Med Pathol Oral Radiol Endod 2008;105:606–616. [CrossRef] [PubMed] [Google Scholar]
- Buchner A, Hansen LS. Amalgam pigmentation (amalgam tattoo) of the oral mucosa. A clinicopathologic study of 268 cases. Oral Surg Oral Med Oral Pathol 1980;49:139–147. [CrossRef] [Google Scholar]
- Amano H, Tamura A, Yasuda M, Yamanaka M, Takeuchi Y, Sasaoka K, et al. Amalgam tattoo of the oral mucosa mimics malignant melanoma. J Dermatol 2011;38:101–103. [CrossRef] [PubMed] [Google Scholar]
- Buchner A. Amalgam tattoo (amalgam pigmentation) of the oral mucosa: clinical manifestation, diagnosis and treatment. Refuat Hapeh Vehashinayim (1993) 2004;21:19–22. [Google Scholar]
- Eisen D. Disorders of pigmentation in the oral cavity. Clin Dermatol 2004;70:682–683. [Google Scholar]
All Figures
|
Fig. 1 A 56-year old man with a large mucosal pigmentation, extending from the right maxillary canine to the tuberosity. |
| In the text | |
|
Fig. 2 Histological section of the palatal mucosa. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.