| Issue |
J Oral Med Oral Surg
Volume 27, Number 1, 2021
|
|
|---|---|---|
| Article Number | 11 | |
| Number of page(s) | 5 | |
| DOI | https://doi.org/10.1051/mbcb/2020050 | |
| Published online | 08 December 2020 | |
Up-to Date Review And Case Report
Rapid prototyping: applications in oral and maxillofacial surgery
1
Department of Maxillo-Facial Surgery, Hospital of Perugia, Sant'Andrea delle Fratte, 06132 Perugia, Italy
2
Department of Medicine, Section of Maxillo-Facial Surgery, University of Siena, Viale Bracci, 53100 Siena, Italy
3
Department of Medicine, University of Perugia, Piazzale Gambuli 1, 06129 Perugia, Italy
4
Paediatric Dentistry Post-graduate School, University of Rome “Tor Vergata”,Via Montpellier 1, Roma, Italy
5
Department of Surgery and Biomedical Sciences, Section of Maxillo-Facial Surgery, University of Perugia, Piazzale Gambuli 1, 06129 Perugia, Italy
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
9
February
2020
Accepted:
26
August
2020
Abstract
This article documents four mandibular reconstructions performed using free fibula flaps. CT scan DICOM (Digital Imaging and COmmunication in Medicine) files were obtained in order to print stereolithographic models of the mandible, and in one case cutting guides for fibular osteotomies. One case study details the treatment a cancer recurrence on a right emimandibulectomy. Because of a lack of access to previous CT scans, the left part of the mandible was mirrored to obtain an accurate 3D model. In one case, due to the young age of the woman, a double barrel fibula flap was used. All cases resulted in satisfactory chewing function and aesthetic outcome, with no flap failures. The report concludes that Virtual Planning and Rapid Prototyping are helpful as they reduce costs and intraoperative times while simultaneously improving surgical precision.
Key words: Mandibular reconstruction / rapid prototyping / stereolithographic model
© The authors, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Reconstruction has emerged as a standard treatment for complex fractures and neoplasms. These are challenging procedures, especially for defects in the head or neck. Here it is important to consider the functional, aesthetic and psychosocial impacts of reconstructive surgery.
Rapid Prototyping (RP) techniques allow physical models to be made from data. Fused Deposition Modelling (FDM) and stereolithography (SL) are RP techniques beneficial to medicine. They have wide ranging applications with respect to orthopedic, maxillofacial, neurological and thoracic surgical procedures [1]. This article discusses their applications to maxillofacial surgery. The RP procedure begins with data acquisition [2], the operations documented here acquired data from CT scans. This is more common than the usage of MRI or ultrasound, although these are also possible data sources. The data is converted into a computer model and 3D printed to output a physical model. Processing software can be used to aid tissue selection by superimposing CT scans of various parts of the body. Although both hard and soft tissues can be constructed, hard tissues are more commonly manufactured due to their intrinsic bone structure. This report presents four cases of mandibular reconstruction, and discusses the management of the 3D models. Especially we want to focus the attention on the short time needed to complete the reconstruction plan and get the 3D models in comparison to other methods.
Methods
Four patients treated in our department will be discussed in this report. In all cases data acquisition was performed by Computed Tomography. CT scans were performed in environments external to the hospital, the parameters of acquisition were not standardised. CT data was acquired as DICOM images and processed by an external company. All cases were discussed with the external specialist to explain the clinical case and formulate our requests. The DICOM data was processed and exported as a 3D-printable STL file. In all cases the RP technology of choice was stereolithography. The 3D models and surgical cutting guides were available within 48 h of the data being sent. The virtual design allowed the projection of the surgery and enabled the simulation of various possibilities. The 3D anatomical models were used to better understand the 3D volumes, to validate the final program and pre-plating in order to reduce the operative times. The 3D-printer used was the Formlabs model “Form2”. Because of the resin thermoplasticity, all the pieces were gas-plasma sterilized.
Case series
Case 1
A 43 year old male was admitted with an oral squamous cell cancer (G1) of the right retromolar region. RMN scans showed extension toward the infratemporal fossa and mandibular ramus. We performed a right hemimandibulectomy, comprehensive of the condyle to the element 45 included, masticatory muscles and extended up to the skull base. The patient was young and without comorbidity so a mandibular reconstruction was mandatory. A left fibula osteo-cutaneous flap was chosen. A stereolithographic model of the mandible was constructed based on CT scans. The superimposition of the fibula flap on the mandible allowed the reconstructive segments' positioning to be checked. The model was employed the day before surgery to plan the osteotomy. It was used to pre-bend the plates, create a cutting guide and measure the fibula segments. In order to reduce the volume of implantable material, two short plates were used instead of a unique plate along the full flap length. The model was gas plasma sterilised and used intraoperatively for procedural verification. The postoperative CT scan shows that the fibula bone segments have good orientation and optimal apposition. The new condyle was fixed by a loose wire to the glenoid fossa to ensure a normal range of motion. The four month follow-up reported stable fibular segments and satisfactory mandibular movement. The implant-prosthetic rehabilitation phase was planned for the upcoming months (Fig. 1a–c).
 |
Fig. 1 (a) Preoperative TC scan; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
Case 2
A 47 year old male admitted with a mandibular squamous cell (G2) cancer. The cancer was centred on the elements 45–46 region and extended to the mandibular bone and vestibular soft tissues (pT4a N0). A mandibulectomy was performed. This was extended from element 43 included to the mandibular right angle, comprehensive of part of the oral pelvis and vestibular soft tissues. The surgical defect was reconstructed by an osteo-cutaneous fibula flap. An engineer was consulted to plan the osteotomies on the mandible and validate the final program. As in the previous case, we validated the program after checking the fibula segments' orientation by superimposing them on the mandible CT images. A 3D model of the patient's mandible was printed from the preoperative CT images. The fibula flap was cut into two segments in order to reproduce the original mandibular anatomy. The model was used to bend the reconstructive plate. Space was left for three holes in the mandibular ramus and symphysis. The optimal length was found for the screws. The contoured plate underwent standard sterilisation and the anatomical mandible model was sterilised by gas plasma. The model was used for the verification of reconstructive phases during surgery. The postoperative CT scans show a good bone apposition between the two fibula segments; and also between the fibula and the ramus and symphysis. The follow up patient shows preserved occlusion (Fig. 2a–c).
 |
Fig. 2 (a) Preoperative TC scan; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
Case 3
A 46 year old female was admitted complaining about swallowing of the anterior mandibular region. The CT scans showed an expansive mass deforming the vestibular cortical bone of the mandible. This mass was centred on the premolar right region. The definitive histopathological diagnosis refers to a squamous cell G1 carcinoma. A mandibular resection was performed. This included teeth from element 42 to the mandibular right angle. As the patient was young the mandible could be constructed with a double barrel free fibula flap. CT scans were acquired; the resection of the mandible and the position of the fibula flap segments were simulated with the superimposition technique. A stereolithographic model was created and used to bend the recon plate the day before surgery. The model was sterilised by gas plasma while the plate by the standard sterilisation cycle. The left fibula flap was segmented in three parts to reconstruct the mandible. Two standard miniplates were used to fix the superior segment to the inferior segment. The postoperative CT scan shows a good bone apposition, an effective fixation by a reconstruction plate extended since the symphysis to the mandibular ramus. The next step is implant-prosthetic rehabilitation. This should aid chewing and provide a better aesthetic outcome (Fig. 3a–c).
 |
Fig. 3 (a) Preoperative intraoral photo; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
Case 4
A 75 year old female with a squamous cell G2-G3 oral cancer recurrence. Two years earlier she had undergone a right hemi-mandibulectomy extended from the condyle to the mentalis foramen for a right retromolar region cancer. She was reconstructed by a pectoralis major pedicled flap, with no mandibular bone reconstruction. As the recurrence was isolated without distant metastases, a salvage surgery was performed. This extended the hemi-mandibulectomy since de right mentalis foramen region to the left mentalis foramen region. Because of the previous hemi-mandibulectomy and soft tissue scar retraction it was impossible to directly print a useful 3D model of the mandible. Furthermore a CT scan showing the full mandible could not be found. It was therefore necessary to use the mirroring technique. A specialist mirrored the left mandible to produce a full mandible. Because of the muscles and scar retraction, the mandible was mirrored using the face median sagittal axis instead of the mandibular median sagittal axis. This was to have the mirrored condyle head in the correct position in the glenoid fossa. The left mandible rotation would have positioned the condyle in an incorrect position using the median sagittal mirroring axis of the mandible. Validated by virtual planning, the 3D model project was finally exported in STL format and printed. It was used to pre-bend the reconstructive plate. A fibular osteo-cutaneous flap segmented in two pieces was chosen to reconstruct the mandible symphysis and body. In order to reduce intraoperative times the condyle was not reconstructed. Thanks to an accurate virtual program, a good mandibular projection and facial symmetry were obtained (Fig. 4a–e).
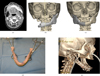 |
Fig. 4 (a) Preoperative TC scan; (b) mandible mirroring 1; (c) mandible mirroring 2; (d) stereolithographic model and reconstructive plate; (e) postoperative TC scan. |
Discussion
Reconstructive surgery of the head and neck has always been a difficult challenge. The complexity of the region has required a high degree of precision for satisfactory outcomes. When jaws were involved it was necessary to preserve the masticatory function with teeth occlusion [3]. Another aim was to achieve acceptable facial symmetry, sometimes by reconstructing the lost tissue with another as similar as possible, thus reducing psychosocial discomfort. Contemporary surgeons have employed virtual surgical planning. The efficiency of virtual planning has improved precision and saved time [4]. When high precision was required (for example in fibular implant supported dental prosthesis), accurate virtual planning of the implant positioning modulated on the fibular segments' orientation achieved more satisfactory results. Correct virtual planning and the RP of a surgical guide led to optimal implant positioning, reducing failure rates and operative times [5]. The rigid fixation of the bony component of the free flaps remains a risky procedure with a 10–15% plate removal rate [6–8]. It can be difficult to choose between standard fixation miniplates, reconstruction and custom-made plates. Zhang et al. found that miniplates and reconstruction plates to be suitable for osteo-cutaneous flap fixation reconstructing the mandible; no significant difference in complication rates were reported [9]. Zavattero et al. chose miniplate fixation because of the minimal metal inserted in comparison to reconstruction or custom-made plates [10]. We do not use custom made preformed plates in malignant neoplasms. Miniplates and reconstruction plates are preferred as they have been found to be more adaptable when the preoperative surgical excision plan has needed to be changed during surgery.
Pre-shaping plates on a 3D stereolithographic model has given the same precision in terms of anatomical adaptation of the plates to the bone as custom-made plates [10]. In cases where the CT scan has underestimated the cancer extension or R+ intraoperative margins, custom made plates and cutting guides have become useless as they have not allowed any change in the plan. Using traditional reconstruction plates or miniplates has proven more agile as surgery plans have been readily changed in response to developing information. Complete custom made surgical plans with custom made guides and plates have often taken longer to be prepared, causing delays. A complete custom-made plan usually takes 7–14 days before the materials are ready; stereolithography only requires 2 working days. There have also been considerable economic advantages. A complete custom-made plan costs $7000 or more while RP programs costs only $600–700. Costs were cut further when RP was implemented in-house by the surgeon [11,12]. The cases discussed above have demonstrated that shaping plates with a 3D model is a successful method for bone segments fixation. There were no recorded complications with plate removal or bone segment stability, even in patients who underwent radiotherapy postoperatively. The flexibility of RP techniques allow the printing of cutting guides, for both the free flap harvest and the ablative phase. It has also allowed for pre-surgery simulation for verification. The possession of 3D models before surgery allows for further scrutiny of the reconstruction plan than that which can be achieved with a PC monitor alone. 3D printing is able to reduce intraoperative times and the possibility of human error. There can be more precise ablative and reconstructive phases. This is due to simulation, and the modification of the dimensions and orientation of the segments [12,13].
Conclusions
RP technologies are widely used, and their utility is discussed in literature. They reduce intraoperative times and mitigate the risk of making errors in harvesting bone flaps and in the ablative phases. The reduced costs, the short time in acquisition of the RP models and the possibilities “to see and touch” the anatomical model before the operative day give to the RP technologies an important role in the reconstruction of the head and neck district.
Ethical approval and patient consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the Helsinki declaration of 1975. Informed consent was obtained from all patients for being included in the study
Conflicts of interests
The authors declare that they have no conflicts of interest in relation to the publication of this article.
References
- Winder J, Bibb R. Medical rapid prototyping technologies: state of the art and current limitations for application in oral and maxillofacial surgery. J Oral Maxillofac Surg 2005;63: 1006–1015. [CrossRef] [PubMed] [Google Scholar]
- Mankovich NJ, Cheeseman AM, Stoker NG. The display of three-dimensional anatomy with stereolithographic models. J Digit Imag 1990;3:200. [CrossRef] [PubMed] [Google Scholar]
- Brown JS, Shaw RJ. Reconstruction of the maxilla and midface: introducing a new classification. Lancet Oncol 2010;11: 1001–1008. [CrossRef] [PubMed] [Google Scholar]
- Ganry L, Hersant B, Quilichini J, Leyder P, Meningaud JP. Use of the 3D surgical modelling technique with open-source software for mandibular fibula free flap reconstruction and its surgical guides. J Stomatol Oral Maxillofac Surg 2017;118:197–202. [CrossRef] [PubMed] [Google Scholar]
- Freudlsperger C, Bodem JP, Engel E, Hoffmann J. Mandibular reconstruction with a prefabricated free vascularized fibula and implant-supported prosthesis based on fully three-dimensional virtual planning. J Craniofac Surg 2014;25:980–982. [CrossRef] [PubMed] [Google Scholar]
- Day KE, Desmond R, Magnuson JS, Carroll WR, Rosenthal EL. Hardwere removal after osseous free flap reconstruction. Otolaryngol Head Neck Surg 2014;150:40–46. [CrossRef] [PubMed] [Google Scholar]
- Wood CB, Shinn JR, Amin SN, Rohde SL, Sinard RJ. Risk of plate removal in free flap reconstruction of the mandible. Oral Oncol 2018;83:91–95. [CrossRef] [PubMed] [Google Scholar]
- Knott PD, Suh JD, Nabili V, et al. Evaluation of hardware-related complications in vascularized bone grafts with locking mandibular reconstruction plate fixation. Arch Otolaryngol Head Neck Surg 2007;133:1302–1306. [CrossRef] [PubMed] [Google Scholar]
- Zhang ZL, Wang S, Sun CF, Xu ZF. Miniplates versus reconstruction plates in vascularized osteocutaneous flap reconstruction of the mandible. J Craniofac Surg 2019;30:e119–e125. [CrossRef] [PubMed] [Google Scholar]
- Zavattero E, Fasolis M, Garzino-Demo P, Berrone S, Ramieri GA. Evaluation of plate-related complications and efficacy in fibula free flap mandibular reconstruction. J Craniofac Surg 2014;25: 397–399. [CrossRef] [PubMed] [Google Scholar]
- Taylor EM, Iorio ML. Surgeon-based 3D printing for microvascular bone flaps. J Reconstr Microsurg 2017;33:441–445. [CrossRef] [PubMed] [Google Scholar]
- Yuan X, Xuan M, Tian W, Long J. Application of digital surgical guides in mandibular resection and reconstruction with fibula flaps. Int J Oral Maxillofac Surg 2016;45: 1406–1409. [CrossRef] [PubMed] [Google Scholar]
- Robiony M, Salvo I, Costa F, et al. Virtual reality surgical planning for maxillofacial distraction osteogenesis: the role of reverse engineering rapid prototyping and cooperative work. J Oral Maxillofac Surg 2007;65:1198–1208. [CrossRef] [PubMed] [Google Scholar]
All Figures
|
Fig. 1 (a) Preoperative TC scan; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
| In the text | |
|
Fig. 2 (a) Preoperative TC scan; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
| In the text | |
|
Fig. 3 (a) Preoperative intraoral photo; (b) stereolithographic model and reconstructive plate; (c) postoperative TC scan. |
| In the text | |
|
Fig. 4 (a) Preoperative TC scan; (b) mandible mirroring 1; (c) mandible mirroring 2; (d) stereolithographic model and reconstructive plate; (e) postoperative TC scan. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.