| Issue |
J Oral Med Oral Sug
Volume 24, Number 3, 2018
|
|
|---|---|---|
| Page(s) | 119 - 121 | |
| Section | Cas clinique / Short case report | |
| DOI | https://doi.org/10.1051/mbcb/2018005 | |
| Published online | 10 October 2018 | |
Short Case Report
An unusual case of microcystic lymphatic malformation discovered after wisdom teeth extraction
1
University Hospital Center, Clermont-Ferrand, Department of Odontology,
63003
Clermont-Ferrand, France
2
University Hospital Center, Department of Stomatology, Maxillofacial Surgery, and Facial Plastic Surgery,
63003
Clermont-Ferrand, France
3
University of Clermont Auvergne, Neuro-Dol, BP 10448, 63000, Clermont-Ferrand & Inserm U1107,
63001
Clermont-Ferrand, France
* Correspondence: laurent.devoize@udamail.fr
Received:
8
December
2017
Accepted:
28
March
2018
Lymphangioma is a benign vascular malformation of the lymphatic vessels. In 90% of cases it is diagnosed during the first 2 years of life. As seen in 75% of cases, the head and neck region are the preferred location. This report represents an original case of lymphatic malformation (LM) in a 15-year-old patient discovered during an unscheduled postoperative symptomatology of third molar germectomies. Two biopsies, one non-contributory, were required to make the diagnosis. Lymphangiomas are classified as LM. They are usually non-regressive. Their etiology remains controversial.
Key words: lymphangioma / vascular abnormalities / oral cavity / Clinical observation
© The authors, 2018
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Clinical observation
Miss T.A, age 15, had a medical history of chilblains with distal extremity necrosis and was referred by her attending oral surgeon who performed extractions of her four wisdom teeth for orthodontic reasons. The procedure was successful and postoperative management was uneventful.
Three months after the surgery, the patient had an emergency consultation due to the appearance of a painless swollen area at site 48. Palpation led to the pooling of a clear liquid in an area distal to no. 47 where a periodontal pocket had formed.
We rescheduled an outpatient procedure under sedation to perform an alveolar curettage of 48, a fistula tract excision, and to collect a sample for bacterial culture.
The histopathological examination contributed little to the diagnosis, suggesting the possibility of a granuloma consisting of polymorphous inflammatory elements with numerous multinucleated giant cells, which appeared to be resorptive. The bacteriological culture showed the presence of polymicrobial flora and leukocytes.
The patient returned for a consultation after the fistula reappeared on the right retromolar trigone located in the scar tissue area. (Fig. 1).
Another biopsy was performed, which revealed dilated lymphatic cavities with anfractuous light on the chorion’s surface. The cavities contained fibrin, some macrophages, some polynuclear cells, and rare red blood cells. The cavity walls were thin with some areas of newly-formed capillaries and collagen fibrosis. On the surface, a well-differentiated non-keratinized stratified squamous epithelium was found.
Its histological appearance suggested the presence of a microcystic lymphatic malformation (LM) (Fig. 2) of <1-cm diameter with mucosal involvement.
Different treatment options were proposed to both the patient and her parents, including conservative management, sclerotherapy, electrocoagulation, and surgery. For now, the patient has chosen conservative management and regular follow-ups. At 24 months, the LM was still present but had not progressed.
 |
Fig. 1 Lymphatic malformation of the right retromolar trigone. A translucent vesicular lesion next to the distovestibular cuspid of 47 is noticeable. The fact that it appears to be healing indicates that no further investigation is necessary. |
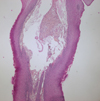 |
Fig. 2 Histological section (×4) stained with hematoxylin–eosin saffron (HES): A large, dilated, lymphatic cavity accompanied by smaller histologically similar cavities is observed. |
Discussion
According to the 1996 International Society for the Study of Vascular Anomalies classification scheme by Mulliken et al., which was recently updated in 2014, lymphangiomas and hemolymphangiomas should both be referred to as LM.
Representing 6% benign tumors found in children [1]. They can evolve during inflammatory episodes, intracystic hemorrhages, or cavity infections. They do not have the tendency to spontaneously regress.
LM of the oral mucosa are rare. The most common location is the mobile part of the tongue, followed by the palate, gums, or lips. They are mostly superficial. The vesicles often have a translucent appearance and may occasionally appear red or blue after the rupture of the capillaries that pass through the lymphatic spaces.
Its gingival location and translucent appearance is clearly visible in the intraoral photograph (Fig. 2).
There are two clinical forms of LM—macrocystic and the microcystic (or tissue). Each form has different treatments and prognosis. The macrocystic LM is usually occurs in the neck and is a well-defined, fluctuant swelling, covered by normal-colored skin. The microcystic form, diagnosed in our patient, is preferentially located on the tongue and cheek. However, it typically appears as a poorly-defined, subcutaneous or mucosal swelling, covered with raised sacs (vesicles) on the skin that contain clear or bloody (hemorrhagic) fluid [2]. The microcystic and macrocystic LMs can be easily distinguished on MRI due to their size difference and cystic components.
A subclassification has been described in the literature:
-
capillary LM, which involves small capillary vessels;
-
cystic LM which consists of large, macroscopic, cystic spaces [3];
-
and cavernous LM, composed of large, dilated lymphatic vessels.
The most common oral form is cavernous LM.
The presence of the skeletal muscles and the dense connective tissue in the oral cavity prevent the lymphatic vessels from expanding; therefore, the malformation remains superficial and mostly asymptomatic. In the case of deep lesions, they are generally described as voluminous masses with a diffuse growth pattern causing various mass-effect symptoms: upper airway obstructions, deformation of the jaws, compression pains, lingual extrusion, hypersialorrhea, as well as difficulties during oral hygiene, speech, and mastication.
The patient’s age, along with the lesion’s location, volume, symptomatology, and locoregional impact are the main factors influencing the therapeutic decision [4].
Interventional therapies are aesthetic, functional, or motivated by chronic pain symptoms [2].
-
The CO2 laser is widely used in the oral cavity because of its affinity for water and its high absorption by the oral mucosa. It is used to treat small, superficial lesions, and healing is often faster with few postoperative complications [5];
-
OK-432 (Picibanil) is a commonly used sclerosing drug. After it is injected, an active local reaction ensues, which progresses to inflammation, fibrosis, and lesion healing. The literature on sclerotherapy of LM provides very little evidence and lacks standardization [6]. In addition, no previous study has directly compared surgical therapies with sclerotherapy [7].
Surgical excision remains the gold standard for treating these malformations. Nevertheless, because of their non-encapsulated and infiltrative nature, complete excision of lymphangiomas remains difficult [3].
Conflict of interest
The authors declare that they have no conflicts of interest in relation to this article.
References
- Pierrot S, Manach Y, Couloigner V. Cervicofacial lymphangiomas: imaging, diagnosis and treatment. EMC − Oto-Rhino-Laryngol 2011;6:1–7. [CrossRef] [Google Scholar]
- Rochefort J, Lescaille G, Hervé G, Agbo-Godeau S, Mauprivez C. Oral lymphatic malformations, case reports and review of the literature. Med Buccale Chir Buccale 2017;23:51–59. [CrossRef] [Google Scholar]
- Sunil S, Gopakumar D, Sreenivasan BS. Oral lymphangioma − case reports and review of literature. Contemp Clin Dent 2012;3:116–118. [CrossRef] [PubMed] [Google Scholar]
- Wassef M, Blei F, Adams D, Alomari A, Baselga E, Borenstein A. Vascular anomalies classifcation: recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics 2015;136:e203–e214. [CrossRef] [PubMed] [Google Scholar]
- Colbert SD, Seager L, Haider F, Evans BT, Anand R, Brennan PA. Lymphatic malformations of the head and neck—current concepts in management. Br J Oral Maxillofac Surg 2013;51:98–102. [CrossRef] [PubMed] [Google Scholar]
- Churchill P, Otal D, Pemberton J, Ali A, Flageole H, Walton JM. Sclerotherapy for lymphatic malformations in children: a scoping review. J Pediatr Surg 2011;46:912–922. [CrossRef] [PubMed] [Google Scholar]
- Adams MT, Saltzman B, Perkins JA. Head and neck lymphatic malformation treatment: a systematic review. Otolaryngol Head Neck Surg 2012;147:627–639. [CrossRef] [PubMed] [Google Scholar]
All Figures
|
Fig. 1 Lymphatic malformation of the right retromolar trigone. A translucent vesicular lesion next to the distovestibular cuspid of 47 is noticeable. The fact that it appears to be healing indicates that no further investigation is necessary. |
| In the text | |
|
Fig. 2 Histological section (×4) stained with hematoxylin–eosin saffron (HES): A large, dilated, lymphatic cavity accompanied by smaller histologically similar cavities is observed. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.