| Issue |
J Oral Med Oral Surg
Volume 31, Number 1, 2025
|
|
|---|---|---|
| Article Number | 2 | |
| Number of page(s) | 5 | |
| DOI | https://doi.org/10.1051/mbcb/2025004 | |
| Published online | 18 February 2025 | |
Case Report
Giant dermoid cyst of the buccal floor: a case report
Service ORL, CHU Félix Guyon, 974 00 Saint Denis, La Réunion, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
28
May
2024
Accepted:
21
January
2025
Abstract
Dermoid cysts of the buccal floor are uncommon lesions, typically found in young individuals. Herein, we report the case of a 15-year-old patient referred by her general practitioner after MRI evaluation. The patient complained of dysphagia with solid foods and aesthetic discomfort due to a swelling under her chin, which led to teasing at school. She exhibited no signs of severity. Imaging revealed a sizable buccal floor cyst measuring 7 cm × 4 cm × 3 cm. Surgical excision was performed via a dual approach, intraoral and cervical, with straightforward postoperative recovery. Histopathological analysis confirmed the diagnosis of a dermoid cyst. Management of dermoid cysts remains exclusively surgical, with rare recurrences dependent on complete excision quality. Prognosis is favorable.
Key words: Dermoid cyst / buccal floor
© The authors, 2025
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Dermoid cysts of the buccal floor are rare lesions, occurring in approximately 1–1.6% of cases [1]. They predominantly affect young individuals, typically discovered during the second and third decades of life. While they develop slowly, they can reach significant sizes and interfere with functions such as speech and swallowing, and ultimately present respiratory risks for patients. Diagnosis of these cysts presents challenges, as do surgical and anesthetic issues.
Observation
A 15-year-old female, accompanied by her father, presented for evaluation of a submental swelling with no significant medical history or known allergies.
This swelling had been present at least since April 2023, prompting consultation with her general practitioner who subsequently referred her for an MRI to ear, nose and throat (ENT) and cervico-facial surgery department at CHU Felix Guyon in Reunion Island.
She described episodes of submental swelling and regressions without infectious complications. There was no associated pain, though she experienced mild dysphagia with solid foods. She could tolerate food intake without difficulty and exhibited no dyspnoea. Her father reported significant snoring. She had been experiencing dysarthria for five months with no associated dysphonia.
Clinical examination of the face (Fig. 1) revealed a submental swelling, present anteriorly and laterally with a double chin aspect. Upon palpation, the collection felt soft/depressible (fluid-filled).
Oral cavity examination (Fig. 2) revealed buccal floor swelling, pushing the tongue downwards. The covering mucosa appeared healthy.
Oropharynx examination was challenging. Clear saliva flow was observed bilaterally at the submandibular duct orifices upon pressure over the submaxillary glands. These glands were soft, non-tender, and not enlarged.
Dental examination was unremarkable, with no pain, dental mobility, or periodontal inflammation. The patient exhibited anterior maxillary and mandibular crowding.
Nasofibroscopy revealed normal pharyngeal mucosa. However, the airway was narrowed by the basal bulge on the tongue, potentially explaining the snoring. The larynx appeared normal, and the respiratory tract was patent.
In MRI Imaging in T2 weighting, an oval-shaped cystic formation (Fig. 3) was identified at the buccal floor, with thin walls and fluid content. This formation measured 7 cm in height, 4 cm in anteroposterior diameter, and 3 cm in width, with a double convexity at its base. The mylohyoid and geniohyoid muscles appeared displaced externally (Fig. 4).
Surgical intervention under general anaesthesia was decided. An intraoral approach was initially chosen (Fig. 5). An incision was made at the buccal floor mucosa using monopolar electrocautery, followed by cyst dissection using manual and blunt dissection techniques. Preservation of important anatomical structures, such as lingual nerves and submandibular duct, was ensured. Due to the cyst's basal extension, wider than the mandibular arch, it was complex to completely encircle it intraorally. Hence, a complementary cervical approach was required. A 5cm median incision was made, 1cm above the hyoid bone, passing beneath the platysma and between the anterior bellies of the digastric muscles, then opening the mylohyoid muscle to dissect the cyst's base. The two incisions were connected, and the tumor was delivered (Fig. 6). The cyst was sent for histopathological analysis. A cervical drain was placed. Closure was performed in two layers, intraorally and cervically. The postoperative course was uneventful, with the resumption of a smooth diet on the same evening. An 8-day course of amoxicilline and clavulanic acid association antibiotic therapy was initiated.
Postoperative course: The postoperative recovery was uncomplicated, and the pain was managed with first-line painkillers. The cervical scar was closed within about ten days. The buccal scar was unremarkable, but there remained an induration in the buccal floor ten days after the procedure. This completely disappeared after a few weeks. There was sensory paralysis of neither the tongue nor the floor of the mouth. No Submandibular gland swelling nor pain. Clinically, there is no longer a double chin appearance, and dysphagia and dysarthria were resolved.
Histopathological analysis: The cyst had a granular content. The images showed a cystic formation with a wall composed of a complete squamous epithelium featuring a granular layer. The cyst lumen was filled with keratin lamellae. The surrounding connective tissue was fibrous. There was no significant inflammatory remodeling. This analysis was compatible with a large dermoid cyst of the epidermoid type. No signs of malignancy was found.
 |
Fig. 1 Clinical profile examination showing swelling under the chin. |
 |
Fig. 2 Swelling of the floor of the mouth pushing the tongue towards the floor. The covering mucosa is healthy. |
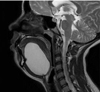 |
Fig. 3 Profile MRI in T2 weighting. |
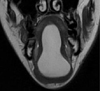 |
Fig. 4 Geniohyoid and mylohyoid muscles pushed by the cyst in T2 weighting. |
 |
Fig. 5 Endobuccal approach, dissection in contact with the cyst while respecting the lingual nerve. |
 |
Fig. 6 Excision of the cyst via cervical approach. |
Discussion
Dermoid cysts pose diagnostic challenges, especially in differentiating them from lingual, submental, and cervical masses. The mucoid cyst of the sublingual gland, known as “ranula”, is covered with a thin mucosa exhibiting a bluish coloration and evolves through a fistula (containing liquid content). It is a painless lesion [2].
The dermoid cyst is also painless, with a thicker, pasty, lumpy, whitish content. The covering mucosa appears healthy.
Branchial cysts, fistulas or sinuses are developmental abnormalities resulting from incomplete closure of branchial clefts or pouch [3]. These are lateral neck abnormalities not middle line ones such as our case report. A sinus (« incomplete fistulae ») is formed when the tract is open either to the pharynx or to the skin. A cyst is formed when there is no communication to either of the two. It can however be associated with a sinus or a fistula. A branchial fistula forms when there is a remnant of both the pouch and the cleft [4].
Those of the first cleft are rare and located in the Poncet triangle (between the tragus, the mental symphysis, and the hyoid bone). Second cleft cysts are by far the most common branchial anomalies. They are usually located in the lateral neck infrahyoid and anterior to the sternocleidomastoid muscle. The majority of cases arise in young patients between 20 to 40 yr of age although branchial cleft cysts can present in infants and young childrens. Fistulae or sinuses are more diagnosed in first stages of life. A second branchial cleft fistulae connect his external skin opening to the oropharynx at the tonsilar fossa. Third and fourth cleft cysts, sinuses or fistulas are rare, reported more commonly on the left side, with the skin opening, if present, between the inferior middle to the medial lower third border of the SCM near the supraclavicular region. They are in close relationship with the thyroid gland and fistulas or sinuses are opened in the pyriform sinus [5].
Lipomas are soft swellings with a characteristic yellow appearance; in the oral cavity, they are most often located in the cheek and then in the buccal floor [6].
An infection like submental cellulitis should be kept in mind. In this case report, there were no dental symptoms: no carious or traumatic dento-alveolar lesion and no signs of percussion pain on the mandibular anterior teeth nor mobility of them. Our patient had an old painless mass without any infectious signs.
A malignant lesion is usually poorly defined, ulcerated, budding, palpably indurated, bleeding on contact, and painful. In our case, the mass was a well-delineated cystic lesion without local sign of aggressivity as well in MRI and in his clinical aspects with healthy mucosa and skin on one side or the other. Clinical and Radiological diagnosis didn't let place for doubt. Therefore, we ruled out malignancy.
Cervical masses that may resemble this lesion include a high median thyroid nodule much likely to be in an infrahyoid position. Thyroglossal duct (TGD) cyst are another common congenital midline lesion around the level of hyoid bone due to TGD remnants. It is mandatory to ensure that thyroid gland is in his normal cervical position before surgical excision of TGD cysts. Lingual base of tongue thyroid gland is a rare condition. In case of supra hyoid TGD cyst, they are usually much dorsal, near the pre-epiglottic space and going up to the tongue base and foramen caecum (embryological migration of the thyroid gland in the thyroglossal duct). Here, our lesion is located in the upper midline position (suprahyoid) and is too much anterior to be confounded with a TGD cyst who don't have any relationship with the floor of mouth for later.
Other congenital lesions, such as vascular malformation or lymphangioma (cystic hygroma), are usually included in the differential diagnosis of cervical masses extending to the oral floor. These lesions are smooth, erythematous or bluish and sometimes pulsatile [7]. In these lesions MRI and radiological findings are pathognomonic.
In this case report, the clinical and radiological (MRI) data leaned towards the diagnosis of dermoid cyst of the oral floor, and histopathological analysis confirmed the diagnosis: epidermoid-type dermoid cyst. Histologically, a true dermoid cyst presents a stratified, keratinizing squamous epithelium, as well as skin appendages such as sweat and sebaceous glands, and adnexal structures (hair follicles) [8,9]. In the absence of these appendages or adnexal structures, the lesion is then referred to as an epidermoid cyst [10].
Imaging (CT with contrast/ultrasound/MRI) can be used to visualize the liquid content and extent of the lesion, but MRI remains the preferred examination to assess the cyst's relationship to the mylohyoid and geniohyoid muscles [8]. MRI of dermoid cysts reveals variable signal intensity on T1-weighted images and typical hyperintensity on T2-weighted images. This examination is particularly useful for assessing the relationship between the cystic mass and the muscles of the floor of the mouth [11].
In the literature, the described management is exclusively surgical, with no marsupialization as for mucoid cysts of the oral floor. Moreover, marsupialization could complicate cyst dissection, potentially leaving part of the capsule behind. Complete surgical excision is necessary to prevent recurrence.
Depending on size and location, various approaches are described: the endo-oral approach for sublingual cysts and small ones [12].
The cervical approach is used for cysts exceeding the limits of the geniohyoid and mylohyoid muscles and for large lesions. A combined cervical and endo-oral approach may be useful for voluminous lesions where control by the endo-oral route alone is insufficient [13].
The choice of intubation depends on the lesion's extent: nasotracheal intubation is preferable. In the literature, preoperative tracheotomy [14] may be considered to avoid postoperative complications related to surgery (such as hematoma of the oral floor, postoperative edema). In our case, we opted for management with nasotracheal intubation without fiberoptic intubation because the pharynx was clear. A 48-hour observation was conducted in the department to monitor potential complications (monitoring hematoma of the oral floor). Prognosis is generally good, with recurrence being very rare [15] dependent on complete excision quality.
Conclusion
Diagnosing and treating buccal floor lesions present challenges. A wide spectrum of lesions, from mucocoele to malignancy, can occur in this region. Using modern imaging modalities is crucial for accurate diagnosis before a surgical treatment. Dermoid cysts, benign in nature with exceptionally rare malignant transformation, warrant surgical management tailored to individual clinical scenarios.
Acknowledgments
We thank the surgical team for their contribution in the patient's follow up.
Funding
No funding was received.
Conflicts of interest
The author reports no potential conflicts of interest.
Data availability statement
The data can be shared upon request.
Informed consent
Written informed permission was obtained from the patient to publish this case report and any accompanying images.
References
- Bokoa E, Amaglob K, Kpemissi E. Volumineux kyste dermoïde du plancher buccal. Annales Françaises d'Oto-Rhino-Laryngologie et de pathologie cervico-faciale 2014;131:117–120. [CrossRef] [Google Scholar]
- Wong KT, Lee YY, King AD, Ahuja AT. Imaging of cystic or cyst- like neck masses. Clin Radiol 2008;63:613–622. [CrossRef] [PubMed] [Google Scholar]
- Glosser JW, Pires CA, Feinberg SE. Branchial cleft or cervical lymphoepithelial cysts: Etiology and management. J Am Dent Assoc 2003;134:81–86. [CrossRef] [PubMed] [Google Scholar]
- Boonen A, Hens G, Meulemans J, Hermans R, Delaere P, Vander Poorten FV. Fourth branchial anomalies: Diagnosis, treatment, and long-term outcome. Front Surg 2021;8:748351. [CrossRef] [PubMed] [Google Scholar]
- Coste AH, Lofgren DH, Shermetaro C. Branchial cleft cyst. In: StatPearls [Internet] [Internet. StatPearls Publishing; 2023 [cited 2024 Oct 29]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499914/ [Google Scholar]
- El-Momen MH, Gaafar AH, Magdy EA. Lipomas of the head and neck: Presentation variability and diagnostic work-up. J Laryngol Otol 2006;120:47–55 [PubMed] [Google Scholar]
- Gharaibeh TM, Safadi RA, Rawashdeh MA, Hammad HM. Plunging arteriovenousmal formation in the floor of the mouth: A case report. Br J Oral Maxillofac Surg 2010;48:35–37. [Google Scholar]
- Mahmood S, Moody H. Dermoid, teratorma, choristoma? A rare lesion of the tongue in an adult. Br J Oral Maxillofac Surg 2003;41:117–119. [CrossRef] [Google Scholar]
- Ariyoshi Y, Shimahara M. Magnetic resonance imaging of a submental dermoid cyst: Report of a case. Oral Maxilofac Surg 2003;61:507–510. [CrossRef] [Google Scholar]
- Meyer I . Dermoid cysts (dermoids) of the floor of the mouth. Oral Surg Oral Med Oral Pathol 1955;8:1149. [CrossRef] [PubMed] [Google Scholar]
- Pancholi A, Raniga S, Vohra PA, Vaidya V. Midline submental epidermoid cyst: A rare case. Int J Otorhinolaryngol. 2006;4: 74e 77. [Google Scholar]
- Koizuka I . A case of large dermoid cyst in the floor of the mouth. Auris, Nasus, Larynx 2003;30:137–139. [CrossRef] [Google Scholar]
- Colp R. Dermoid cyst of the floor of the mouth. Surg Gynecol Obstet 1925;40:183. [Google Scholar]
- Raveenthiran V, Sam CJ, Srinivasan SK. A simple approach toairway management for a giant sublingual dermoid cyst. Can J Anaesth 2006;53:1265–1266. [CrossRef] [PubMed] [Google Scholar]
- Longo F, Maremonti P, Mangone GM, De Maria G, Califano L. (Dermoïd) Cysts of the floor of the mouth: Report of 16 cases and review of surgical techniques. Plast Reconstr Surg 2003;112:1560. [CrossRef] [PubMed] [Google Scholar]
Cite this article as: Hibelot D, Doger De Speville E. 2025. Giant dermoid cyst of the buccal floor: A case report. J Oral Med Oral Surg. 31: 2. https://doi.org/10.1051/mbcb/2025004
All Figures
|
Fig. 1 Clinical profile examination showing swelling under the chin. |
| In the text | |
|
Fig. 2 Swelling of the floor of the mouth pushing the tongue towards the floor. The covering mucosa is healthy. |
| In the text | |
|
Fig. 3 Profile MRI in T2 weighting. |
| In the text | |
|
Fig. 4 Geniohyoid and mylohyoid muscles pushed by the cyst in T2 weighting. |
| In the text | |
|
Fig. 5 Endobuccal approach, dissection in contact with the cyst while respecting the lingual nerve. |
| In the text | |
|
Fig. 6 Excision of the cyst via cervical approach. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.