| Issue |
J Oral Med Oral Surg
Volume 27, Number 3, 2021
|
|
|---|---|---|
| Article Number | 42 | |
| Number of page(s) | 4 | |
| DOI | https://doi.org/10.1051/mbcb/2021020 | |
| Published online | 26 August 2021 | |
Case Report
Combined local flap and antrostomy in recurrent oroantral fistula and chronic maxillary atelectasis: a case report
1
Department of Oral Surgery, Dijon Bourgogne University Hospital, 21000 Dijon, France
2
Department of Oral, Plastic, Reconstructive, Maxillofacial and Hand Surgery, Dijon Bourgogne University Hospital, 21000 Dijon, France
a Present address: Department of Oral Surgery, Grand Hôpital de l'Est Francilien, 77600 Jossigny, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
14
December
2020
Accepted:
16
May
2021
Abstract
Introduction: Chronic maxillary atelectasis refers to a persistent volume decrease of the maxillary sinus by inward bowing of its walls. When associated with hypoglobus or enophthalmos, some authors use the term “silent sinus syndrome”. We aimed to report a case of accidental diagnosis of chronic maxillary atelectasis while investigating and treating a recurrent oroantral fistula. Observation: CT imaging showed a large bone defect and stage II chronic maxillary atelectasis. Closure of the oroantral fistula was performed with a combined surgical approach: functional endoscopic surgery and buccal fat pad flap. The follow up at 2 months showed no signs of recurrent oroantral fistula. Commentaries: Chronic maxillary atelectasis is separated into three stages, membranous deformity (stage I), bony deformity (stage II), and clinical deformity (stage III). The term silent sinus syndrome should be abandoned for stage III chronic maxillary atelectasis to allow for better collaboration between medical practitioners. Recurrent oroantral fistulas should be treated with a combined approach including endoscopic antrostomy and local flap. Conclusion: The association of functional endoscopic surgery and buccal fat pad flap were the key to success in this case allowing for oroantral fistula closure and treatment of chronic maxillary atelectasis.
Key words: Oroantral fistula / maxillary antrum / oral surgery
© The authors, 2021
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Chronic maxillary atelectasis (CMA) refers to a persistent volume decrease of the maxillary sinus by the inner bowing of its walls. CMA's staging system varies from a membranous deformity (stage I), bony deformity (stage II), to clinical deformity (stage III) [1]. A similar diagnostic is the silent sinus syndrome (SSS) [2].
The pathogenesis of CMA remains unknown, but the main hypothesis is chronic hypoventilation of the maxillary sinus [1,3,4]. Patients consult because of anatomical symptoms (facial deformity) or functional symptoms (sinusitis) [1,3]. In some cases, mild symptoms without CT-scan can lead to misdiagnosis [3].
We aimed to report a case of accidental diagnosis of CMA while investigating and treating a recurrent oroantral fistula (OAF).
Observation
A 74-year-old female patient was referred for a persistent left side OAF with a complaint of a recurrent purulent discharge in the oral cavity. The main medical history consisted of breast cancer treated by surgery (tumorectomy and lymphadenectomy) and external radiotherapy in 2009. The patient had recently stopped smoking. OAF occurred after the extraction of maxillary antral molars (26, 27, and 28). The defect was closed using a buccal advancement flap. But the fistula reappeared two weeks after the operation. Six months later a second surgery (debridement and a buccal advancement flap) performed by another surgeon failed after two weeks. No surgery was done until 18 months later.
Clinical examination showed an OAF measuring 10 mm × 4 mm (tooth 26) (Fig. 1). No diplopia or enophthalmos was diagnosed. A CT-Scan revealed a bone defect measuring 22 mm × 25 mm with bony deformity (stage II CMA) and inward bowing of the medial wall. Lateral and superior walls were thick (Fig. 2). There was an obstruction of the middle meatus confirmed by nasal endoscopy.
The treatment plan was to perform closure of the OAF using a buccal fat pad flap with a concomitant endoscopic middle meatal antrostomy to allow sinus drainage.
Under general anesthesia, firstly, all inflammatory tissues were excised. Secondly, a full-thickness vestibular flap was raised (Fig. 3a). Thirdly, an antrostomy of the middle meatus was performed by nasal fibroscopy (Fig. 3b). Fourthly, the buccal fat pad was dissected and rotated onto the oroantral communication (Fig. 3c). Then, closure of the site was ensured with separate 3-0 absorbable sutures (Fig. 3d).
Antibiotic therapy (Amoxicillin/Clavulanic Acid 1 g/125 mg) was administrated for one week postoperatively, associated with opioids and chlorhexidine mouthwashes.
Follow-up was uneventful after 2 months (Fig. 4).
 |
Fig. 1 Preoperative clinical photograph. Preoperative clinical photograph showing a 10 × 4 mm oroantral fistula on the site of the tooth 26. |
 |
Fig. 2 Midface CT-Scan. Midface CT-scan showing a 22 × 25 mm bone defect on the lateral wall of the left maxillary sinus, and stage II CMA with inward bowing of the medial wall and thickening of the lateral and superior walls. (a) Axial plane. (b) Coronal plane. (c) Sagittal plane. |
 |
Fig. 3 Per-operative photographs. (a) Full thickness flap detachment showing the bone defect. (b) Antrostomy of the middle meatus. The suction canula can be seen through the middle meatus (c) Rotation of the buccal fat pad. (d) Closure with absorbable sutures. |
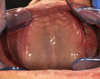 |
Fig. 4 Postoperative clinical photograph. Postoperative clinical photograph at 2 months showing no reopening of the oroantral fistula. |
Commentaries
This case illustrates the importance of maxillary sinus drainage and ventilation. A permeable middle meatus is essential for sinus drainage [5]. An obstructed osteomeatal complex leads to poor ventilation of the sinus. The resulting hypoxia and stasis may lead to sinusitis [6]. Further, hypoventilation of the maxillary sinus is suspected to be the cause of CMA [1,3,4].
The preoperative evaluation of a recurrent oroantral fistula should include tomography imaging to detect any obstructed osteomeatal complex. In our case, the imaging revealed a contracted maxillary sinus and led to the diagnosis of CMA. Several differential diagnoses were discussed and excluded. Because of the absence of spreading process, the well-limited and not osteolytic aspect of the lesion, a nasosinusal malignant tumor was not suspected. Also, a breast cancer metastasis located in maxilla without other locations (lungs, liver or long bones) is very rare [7]. Finally, osteochemonecrosis (OCN) was ruled out because of the absence of medication associated with OCN in the patient's history.
Kass et al. separated the CMA into three stages according to the degree of wall collapse. Stage I refers to membranous deformity with a lateral position of the fontanel and medial infundibular wall. Stage II is characterized by inward bowing of one or more osseous walls. In stage III, the deformation of the antral walls manifests clinically as enophthalmos, hypoglobus, diplopia, or midfacial depression [1].
The therapeutic gold standard to treat CMA is to relieve the obstruction by enlarging the maxillary ostium. This is usually performed under endoscopic sinus surgery [4]. In stage III CMA, reconstruction of the orbital floor can be performed via a transconjunctival or subciliary approach [1].
CMA should be treated in the early stages in order to avoid stage III CMA and orbital floor reconstruction. Anyone commonly confronted with tomography imaging and should be aware of this entity to make the diagnosis at the early stages.
The SSS is very similar to CMA. It is defined by enophthalmos or hypoglobus and ipsilateral maxillary sinus hypoplasia with no associated sinus symptoms [2].
Brandt and Wright [3] proposed to abandon the term silent sinus syndrome and recommended adopting the CMA staging system. There is no significant difference in pathogenesis and no clinical difference other than initial symptomatology between these two entities. The SSS fits very closely to the definition of stage III CMA. This allows for better patient surveillance, better collaboration between medical practitioners and consistency in the literature.
Our patient presented a recurrent OAF with a 25 mm osseous defect. As of today, there is no recommendation on the closure of recurrent OAFs. Multiple techniques have been described to close OAFs, the most accepted being trapezoidal flap, palatal rotation flap, and buccal fat pad flap [8].
The reported failure rate for OAF closure is around 10% depending on the studies, Visscher et al. report a 9.1% failure rate out of 308 patients [9]. It appears that the buccal fat pad flap has the lowest failure rate and causes minimum discomfort when closing OAF larger than 5 mm [10]. The high success rate of this flap may be explained by its rich blood supply: the maxillary artery, the superficial temporal artery, and the facial artery [10].
Recurrent OAFs share common characteristics. Visscher et al. pointed out that maxillary sinusitis at follow up appointment, 10–14 days after OAF closure, was associated with a 15 times higher risk of recurrent OAF [9].
Adams et al. recommend a combined surgery approach to treat oroantral fistulas associated with sinus disease. In Adams' study, closure of the oroantral fistula was obtained with a buccal advancement flap or buccal fat pad flap. Functional endoscopic sinus surgery was performed simultaneously to ensure sinus drainage. The combined success rate was outstanding with 95.5% of the 43 patients showing no dehiscence [11]. This combined approach shows a higher success rate than the one observed by Visscher with 90.9% out of 308 patients treated with a simple OAF closure [9].
In our case, the buccal fat pad was the most secure option given its high success rate, the recurrent aspect of the fistula, and the size of the bone defect. The endoscopic sinus surgery played a double role, treating the CMA and ensuring closure of the persistent oroantral fistula by allowing sinus drainage.
Conclusion
Recurrent oroantral fistula associated with CMA should be treated with a combined approach including local flap and endoscopic antrostomy to ensure closure and avoid recurrence.
Conflicts of interests
The authors have no conflicts of interest to declare.
References
- Kass ES, Salman S, Rubin PA, Weber AL, Montgomery WW. Chronic maxillary atelectasis. Ann Otol Rhinol Laryngol 1997;106:109–116. [CrossRef] [PubMed] [Google Scholar]
- Soparkar CN, Patrinely JR, Cuaycong MJ, et al. The silent sinus syndrome. A cause of spontaneous enophthalmos. Ophthalmology. 1994;101:772–778. [CrossRef] [PubMed] [Google Scholar]
- Brandt MG, Wright ED. The silent sinus syndrome is a form of chronic maxillary atelectasis: a systematic review of all reported cases. Am J Rhinol 2008;22:68–73. [CrossRef] [PubMed] [Google Scholar]
- Blackwell KE, Goldberg RA, Calcaterra TC. Atelectasis of the maxillary sinus with enophthalmos and midface depression. Ann Otol Rhinol Laryngol 1993;102:429–432. [CrossRef] [PubMed] [Google Scholar]
- Beule AG. Physiology and pathophysiology of respiratory mucosa of the nose and the paranasal sinuses. GMS Curr Top Otorhinolaryngol Head Neck Surg 2010;9:Doc07. [PubMed] [Google Scholar]
- Slack R, Bates G. Functional endoscopic sinus surgery. Am Fam Phys 1998;58:707–718. [Google Scholar]
- Namad T, Benbrahim Z, Najib R, Mohammed A, Baggar S, Bouyahia N, et al. Maxillofacial metastasis from breast cancer. Pan Afr Med J. 2014;19:156. [CrossRef] [PubMed] [Google Scholar]
- Franco-Carro B, Barona-Dorado C, Martínez-González MJ, Rubio-Alonso LJ, Martínez-González JM. Meta-analytic study on the frequency and treatment of oral antral communications. Med Oral Patol Oral Cir Bucal 2011;16:e682–e687. [CrossRef] [PubMed] [Google Scholar]
- Visscher SH, van Roon MR, Sluiter WJ, van Minnen B, Bos RR. Retrospective study on the treatment outcome of surgical closure of oroantral communications. J Oral Maxillofac Surg 2011;69:2956–2961. [CrossRef] [PubMed] [Google Scholar]
- Baumann A, Ewers R. Application of the buccal fat pad in oral reconstruction. J Oral Maxillofac Surg 2000;58:389–393. [CrossRef] [PubMed] [Google Scholar]
- Adams T, Taub D, Rosen M. Repair of oroantral communications by use of a combined surgical approach: functional endoscopic surgery and buccal advancement flap/buccal fat pad graft. J Oral Maxillofac Surg 2015;73:1452–1456. [CrossRef] [PubMed] [Google Scholar]
All Figures
|
Fig. 1 Preoperative clinical photograph. Preoperative clinical photograph showing a 10 × 4 mm oroantral fistula on the site of the tooth 26. |
| In the text | |
|
Fig. 2 Midface CT-Scan. Midface CT-scan showing a 22 × 25 mm bone defect on the lateral wall of the left maxillary sinus, and stage II CMA with inward bowing of the medial wall and thickening of the lateral and superior walls. (a) Axial plane. (b) Coronal plane. (c) Sagittal plane. |
| In the text | |
|
Fig. 3 Per-operative photographs. (a) Full thickness flap detachment showing the bone defect. (b) Antrostomy of the middle meatus. The suction canula can be seen through the middle meatus (c) Rotation of the buccal fat pad. (d) Closure with absorbable sutures. |
| In the text | |
|
Fig. 4 Postoperative clinical photograph. Postoperative clinical photograph at 2 months showing no reopening of the oroantral fistula. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.