| Issue |
J Oral Med Oral Surg
Volume 26, Number 1, 2020
|
|
|---|---|---|
| Article Number | 4 | |
| Number of page(s) | 5 | |
| Section | Cas clinique et revue de la littérature / Up-to date review and case report | |
| DOI | https://doi.org/10.1051/mbcb/2019033 | |
| Published online | 23 December 2019 | |
Up-to Date Review And Case Report
Surgical strategy for patients with late-diagnosed minor form of cleidocranial dysplasia: three cases
1
Interne en chirurgie orale, Centre de Chirurgie Orale, Hôpital privé des Cotes d'Armor, 12 Rue François Jacob, 22190 Plérin, France
2
MCU-PH en chirurgie orale, Centre de Chirurgie Orale, Hôpital privé des Cotes d'Armor, 12 Rue François Jacob, 22190 Plérin, France
* Correspondance: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
25
April
2019
Accepted:
29
August
2019
Abstract
Introduction: Cleidocranial dysplasia is a genetic disease affecting bone growth. Observations: 3 patients, aged 12, 14, and 15 followed an orthodontic and surgical treatment to solve an eruption issue of the permanent teeth. Temporary teeth were extracted and impacted teeth were progressively exposed by multiple surgeries under local anesthesia. Anchorages were placed on the teeth and a traction started, on incisors and molars first, then on premolars, and finally on canines. The treatments lasted for 6 to 8 years. Comments: These patients presented minor form of cleidocranial dysplasia which only affected the teeth. The difficulty of these cases lied in the lateness of their diagnosis and treatment. Adaptations had to be made to simplify treatment plans (shortened dental arch, premolar extractions, etc.).
Key words: cleidocranial dysplasia / impacted teeth / treatment
© The authors, 2019
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Cleidocranial dysplasia, or Marie–Sainton syndrome, is a genetic disease characterized by clavicular aplasia, delayed fontanel ossification, and delayed dental eruptions with multiple impactions. The patients described in this article exhibited minor manifestations of this pathology, with exclusive dental involvement that was diagnosed and treated belatedly. The impactions were treated by successive surgeries to facilitate the progressive eruption of the retained teeth. In the present article, three cases are reported and other therapeutic strategies described in the literature are reviewed based on these cases.
Observations
All three patients were orthodontically and surgically treated at the ages of 12 (patient A), 14 (patient B), and 15 (patient C) years. The patients exhibited a significant defect in the eruption of their permanent teeth. The father of the 12-year-old patient as well as the sister of the 15-year-old patient have experienced the same type of impairment but have not undergone treatment (Fig. 1). The patients were initially referred by the orthodontist for avulsion of the residual temporary teeth and disimpaction of the impacted permanent teeth.
The patients did not exhibit any anomalies affecting their clavicles or fontanels. Patient C had a supernumerary tooth (odontoma median to the maxilla).
Initial examinations of the three patients revealed the persistence of several temporary teeth on the arch beyond their normal exfoliation date. The first maxillary molars and a central maxillary incisor were present in the two oldest patients, and the permanent incisor–canine block in the mandible erupted in all patients (Tab. I, Figs. 2–4).
The initial treatment comprised the extraction of the temporary maxillary incisors as well as the disimpaction of the retained permanent maxillary incisors. A mucoperiosteal flap was detached to facilitate anterior access, an alveolectomy was performed to access the crowns of the teeth, and orthodontic brackets were fixed to the vestibular surface to provide tooth traction using interarcade elastics. The flap was closed, with chainette protruding for traction.
For patient A, the subsequent step was the disimpaction of 16 and 26 in the same manner.
Subsequent management consisted of a series of disimpaction surgeries in the following order:
-
The maxillary premolars
-
The first mandibular molars
-
Mandibular premolars
-
Maxillary canines
-
Mandibular canines
The treatments lasted between 6 and 8 years and led to the eruption of most of the teeth retained on the arch (Tab. II). The most frequently observed failure was with regard to the second permanent molars, followed by the permanent premolars, although their absence can compensate for the lack of available space related to the hypodevelopment of the maxilla and mandible (Figs. 5 and 6). The teeth that remained impacted at the end of the treatment were left in place to avoid further intervention.
 |
Fig. 1 Panoramic radiography of patient A's father. He has not had any orthodontic treatment. |
Age of patients and teeth on the arch at the beginning of treatment (temporary teeth are presented in Roman numerals, and permanent teeth are presented in Arabic numerals).
 |
Fig. 2 Clinical view of patient A at the beginning of his treatment (age: 12 years). |
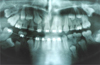 |
Fig. 3 Panoramic radiography of patient A during his treatment (age: 16 years). |
 |
Fig. 4 Panoramic radiography of patient B at the beginning and the end of his treatment (age: 14 and 21 years). |
Age of patients and teeth on the arch at the end of treatment (temporary teeth are presented in Roman numerals, and permanent teeth are presented in Arabic numerals).
 |
Fig. 5 Clinical view of patient C at the beginning of his treatment (age: 15 years). |
 |
Fig. 6 Panoramic radiography of patient C after his orthodontic treatment (age: 23 years). |
Discussion
Cleidocranial dysplasia is an autosomal dominant disease with an estimated prevalence of 1–9/10,00,00,000. The sex ratio is 1, and the disease is linked to mutations in the RUNX 2 (6p21) gene that plays a role in the metabolism of ossification and dentition [1]. The disease is typically characterized by widely open fontanels that remain open throughout life, clavicular aplasia, and dental disorders along with the presence of supernumerary teeth, delay or absence of eruption of the permanent teeth, and presence of associated malocclusions. Some minor manifestations of the disease have been described even if they are rare. There are currently no pathognomonic symptoms [2].
Among the three cases presented, the diagnosis of cleidocranial dysplasia was not evident because only anomalies of the teeth were present. According to the literature, the presence of supernumerary teeth is observed in 93.5% of cases and clavicular hypoplasia in 84.3% of cases [2]. In the absence of a genetic evaluation, the diagnosis of cleidocranial dysplasia by the oral surgeon was based on the fact that these impactions are typical of this pathology. Some less distinct manifestations of the disease are probably underdiagnosed and thus poorly described. Therefore, serious manifestations, with evident diagnosis, have mostly been reported.
Several therapeutic strategies have been described in the literature for the management of dental anomalies related to cleidocranial dysplasia (Tab. III). Most advocate early intervention in anticipation of eruption failure. Therefore, some authors perform movements from 5 to 6 years of age to eliminate temporary teeth and potential obstacles to eruption as well as to expose the anterior teeth early to facilitate the pulling of these teeth under traction using an orthodontic device [1,3,4].
This type of intervention was not feasible in the present cases due to the belated treatment initiation, which was attributable to the lack of knowledge of the treating dentists and orthodontists who referred them. This is more unfortunate for two of the patients as the pathology was present in other members of their family. Therefore, genetic counseling should be provided if the pathology is suspected. It will confirm the diagnosis via genome analysis, coordinate the necessary treatments, and anticipate familial complications [5].
The age of the patients allowed for procedures to be performed under local anesthesia. The primary focus was on the maxillary anterior teeth, which are crucial in restoring an esthetic smile and normal functions (phonation and swallowing). Compromises have occasionally been made (premolar avulsion and temporary teeth preservation) owing to the failure of certain traction mechanisms. In addition, patient fatigue should be considered. In the present cases, the treatments administered were long (between 6 and 8 years) and involved several interventions. In such cases, it is advisable to pay attention to the patient's concerns and respect their choices and modify the treatment plan, if necessary. During adolescence, corticotomies and additional anchoring devices (plates and screws) may help to accelerate results and resolve certain situations where dental support is insufficient.
Summary of different therapeutic strategies to rectify oral impairments of cleidocranial dysplasia in the literature.
4 Conclusion
The age at the time of oral management in patients with cleidocranial dysplasia would probably change the treatment plan. The final goal in the young patient is to rapidly obtain normal teeth. Orthodontic surgical therapy that occurs belatedly must be more pragmatic and open to compromise: short arches, premolar avulsion, and temporary teeth preservation. It must consider the cooperation of the patient who experiences the social and academic repercussions of the absence of permanent teeth as well as the prolonged orthodontic surgical treatment.
Conflicts of interest
The authors declare that they have no conflicts of interest in relation to this article.
References
- Roberts T, Stephen L, Beighton P. Cleidocranial dysplasia: a review of the dental, historical, and practical implications with an overview of the South African experience. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;115:46–55. [CrossRef] [PubMed] [Google Scholar]
- Golan I, Baumert U, Hrala BP, Müssig D. Dentomaxillofacial variability of cleidocranial dysplasia: clinicoradiological presentation and systematic review. Dentomaxillofac Radiol 2003;32:347–354. [PubMed] [Google Scholar]
- Becker A, Lustmann J, Shteyer A. Cleidocranial dysplasia: Part 1-General principles of the orthodontic and surgical treatment modality. Am J Orthod Dentofacial Orthop 1997;111:28–33. [CrossRef] [PubMed] [Google Scholar]
- Becker A, Shteyer A, Bimstein E, Lustmann J. Cleidocranial dysplasia: Part 2-Treatment protocol for the orthodontic and surgical modality. Am J Orthod Dentofacial Orthop 1997;111:173–183. [CrossRef] [PubMed] [Google Scholar]
- Nieminen P. Dental anomalies: genetics. In: John Wiley & Sons, Ltd, éditeur. eLS. Chichester, UK: John Wiley & Sons, Ltd; 2013. [Google Scholar]
- Smylski PT, Woodside DG, Harnett BE. Surgical and orthodontic treatment of cleidocranial dysostosis. Int J Oral Surg 1974;3:380–385. [CrossRef] [PubMed] [Google Scholar]
- Hall RK, Hyland AL. Combined surgical and orthodontic management of the oral abnormalities in children with cleidocranial dysplasia. Int J Oral Surg 1978;7:267–273. [CrossRef] [PubMed] [Google Scholar]
- Berg RW, Kurtz KS, Watanabe I, Lambrakos A. Interim prosthetic phase of multidisciplinary management of cleidocranial dysplasia: “the Bronx Approach”. J Prosthodont 2011;20 Suppl 2:S20–S25. [Google Scholar]
All Tables
Age of patients and teeth on the arch at the beginning of treatment (temporary teeth are presented in Roman numerals, and permanent teeth are presented in Arabic numerals).
Age of patients and teeth on the arch at the end of treatment (temporary teeth are presented in Roman numerals, and permanent teeth are presented in Arabic numerals).
Summary of different therapeutic strategies to rectify oral impairments of cleidocranial dysplasia in the literature.
All Figures
|
Fig. 1 Panoramic radiography of patient A's father. He has not had any orthodontic treatment. |
| In the text | |
|
Fig. 2 Clinical view of patient A at the beginning of his treatment (age: 12 years). |
| In the text | |
|
Fig. 3 Panoramic radiography of patient A during his treatment (age: 16 years). |
| In the text | |
|
Fig. 4 Panoramic radiography of patient B at the beginning and the end of his treatment (age: 14 and 21 years). |
| In the text | |
|
Fig. 5 Clinical view of patient C at the beginning of his treatment (age: 15 years). |
| In the text | |
|
Fig. 6 Panoramic radiography of patient C after his orthodontic treatment (age: 23 years). |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.