| Issue |
Med Buccale Chir Buccale
Volume 23, Number 4, December 2017
|
|
|---|---|---|
| Page(s) | 177 - 180 | |
| Section | Article original / Original article | |
| DOI | https://doi.org/10.1051/mbcb/2017018 | |
| Published online | 22 December 2017 | |
Original Article
One-day hospitalization in oral surgery: a 2-year comparative study
1 Hôpitaux de Paris, France
2 Functional Unit of Oral Surgery and IPES, Hôpital Max Fourestier, Centre hospitalier de Nanterre, France
3 Cardiology Service, Hôpital Max Fourestier, Centre hospitalier de Nanterre, France
4 Diabetology Service, Hôpital Max Fourestier, Centre hospitalier de Nanterre, France
5 Quality and Risk Delegation, Hôpital Max Fourestier, Centre hospitalier de Nanterre, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received: 8 May 2017
Accepted: 1 August 2017
Abstract
Introduction: The increasing number of cardiovascular and/or neurological patients with polypathologic backgrounds has led practitioners to adapt the technical platform. The objective is to evaluate the indications of one-day hospitalization (ODH) in oral surgery set up in 2013 in the Max Fourestier Hospital (Nanterre), a comparative prospective study is carried out in 2014 and 2015. Material and methods: The evaluation criterion is the rate (%) of local or general perioperative complications requiring intervention or full hospitalization of patients at risk for oral surgery with ODH. Results: Sixty-eight interventions were performed, mainly dental extractions, root planning and biopsies. 52% of patients were women. Cardiovascular diseases (36%) were the majority. 20.58% of the included patients had a complication taken up by the practitioner or managed by the day hospitalization service. This rate of complications was statistically significantly different (χ2 = 9.89, P = 5%, NDF = 1) from the control group (3.80%). Discussion: The highest complication rate in polypathologic patients, confirms the indications of ODH. No conversion to full hospitalization was necessary thus this study shows that ODH allows a safe intake taking charge avoiding a full hospitalization of higher cost.
Key words: oral surgery / one-day hospitalization / cardiovascular disease / complication
© The authors, 2017
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
The increasing number of elderly patients with illnesses with cardiovascular and/or neurological comorbidities means that practitioners must adapt their practices to each individual case [1,2]. A working group (cf. Annexes) Of the Max Fourestier Hospital (Nanterre) comprising Odontology service (Dr. H. Tran), Cardiology service (Dr. F. Digne), Diabetology service (Dr. M. Levy) Anesthesia Resuscitation service (Dr. R. Sabbagh) and the day Hospitalization Service (HDJ) of Max Fourestier Hospital (Nanterre) has put in place a care protocol for these patients considered “at risk.” This protocol, according to the reports and recommendations of the la Société Française de Chirurgie Orale et de l'Evaluation des Pratiques Professionnelles (French Society for Oral Surgery and the Evaluation of professional practices) [3,4], aims to supervise and control interventions in these fragile patients. One-day surveillance is an alternative to complete hospitalization. The one-day surveillance allows the patient to return home in the best-case scenario or be admitted to hospital in case of complication [1,2,5]. The objective of this 2-year comparative prospective observational study is to evaluate the rate (%) of perioperative complications in patients at risk with comorbidities and who were operated on in HDJ.
Materials and methods
Outline of the study
This is a prospective study/evaluation that focuses on patients admitted to the Odontology service of Max Fourestier Hospital in 2014 and 2015. The mode of evaluation of therapeutics has been done in a pragmatic way, i.e., by leaving the treatments and interventions as they are usually practiced.
Population
The population consists of patients with multiple pathologies (co-occurrence of at least two chronic diseases over the same period) [2], whose general condition and/or the dental procedure indicates perioperative surveillance. Their free and informed consent is obtained beforehand. The state of their preoperative health is evaluated according to the American Society of Anesthetists (ASA) score (“Physical Status Score”), set up in 1941 by ASA [4,6] according to the severity of the systemic impairment. Patients included in the study are patients classified ASA 1, 2, and 3, the inclusion of ASA 4–6 patients is considered irrelevant.
Inclusion criteria
The general and local criteria, which may be associated or not, are as follows:
General criteria
-
History of frequent discomfort because of hypoglycemia, epilepsy, asthma, and/or arrhythmia;
-
high iatrogenic hemorrhagic risk: (direct oral anticoagulant), anti-vitamin K (AVK) with international normalized ratio (INR) >3, antiplatelet therapy;
-
history of frequent falls;
-
lack of compliance and therapeutic adherence;
-
cognitive impairment;
-
patients under guardianship or curatorship.
Local criteria
-
Dental extraction and multiple implants;
-
dental germectomy;
-
invasive surgeries (extended cysts).
Exclusion criteria
-
Isolated patients (>20 km) indicating a week's hospitalization [1];
-
patients classified ASA 4–6.
The evaluation criterion is the rate (%) of local and/or general perioperative complications requiring a return to the dentist's chair or hospitalization. The local complications are hemorrhage, trauma, or pain. General complications include: malaise, fall, loss of consciousness, seizure, anaphylactic shock, asystole, or death.
Statistical analysis
The comparison of the overall rate (%) of the complications of the group studied with a control group of 78 randomly drawn cases with a table of numbers was made using a qualitative test (χ2). The patients in the control group were randomly selected from the same period as the study group. The interventions conducted out in the control group are comparable to the subjects tested. These are mainly dental extractions. The data were evaluated with an intent to treat. The declaration to the Commission nationale de l'informatique et des libertés (CNIL) [National Commission for Data Processing and Liberties] was made on July 24, 2015 (No. 1876016v0).
Results
The patient (68 interventions in 64 patients) and control (78 interventions in 78 patients) groups were comparable in age (61 ± 10 versus 68 ± 17 years, respectively) and sex (sex-ratio 1:1 in both groups). The interventions in both groups were comparable with the majority (>80%) having undergone dental extractions in the two groups. The average number of teeth extracted was otherwise comparable (2 ± 1 teeth per individual in each group).
Sixty-eight interventions were conducted during the period 2014–2015, in 64 patients aged 67 ± 18 years (age 14–100 years). There were 33 women (52%) and 31 men (48%). Four patients underwent two interventions in the selected period. Individuals aged >65 years with multiple pathologies were predominantly female: 12 women out of 64 (18.75%) versus three men out of 64 (4.68%). The patients who received surgery were in descending order classified as ASA 2, ASA 3, and ASA 1, 50%, 43%, and 7%, respectively (Fig. 1). The pathologies found were mainly cardiovascular (36%), endocrine (32%), neuropsychiatric (12%), other rare diseases (12%), and respiratory (9%) (Fig. 2). An intervention was performed under mélange équimoléculaire oxygène protoxyde d'azote (MEOPA) [equimolecular mixture oxygen protoxide of nitrogen]. The interventions were dental extraction (95.59%, 66/68), extraction/frenotomy (1.47%, 1/68), root planing/extraction (1.47%, 1/68), and biopsy (1.47%, 1/68) (Fig. 3). The rate of complications occurring in the patient group (20%) was significantly different (χ2 = 9.89, P = 5%, DDL = 1) compared with that in the control group (4%) (Fig. 4). The complications were mainly local (87.50%, 14/16): one case of hyperalgesia and 13 cases of hemorrhages: eight under AVK [anti-vitamin K], two under platelet aggregation inhibitor (PAI), and three without treatment. In the patient group, 4% (3/68) of the interventions necessitated a return to the dentist's chair for recovery of hemostasis, whereas none in the control group did (Fig. 3). The remaining 10 hemorrhages could be stopped by the nurse in the HDJ service through compression for 15 min using compresses coated with a tranexamic acid solution (1 g/10 ml). General complications (12.5%, 2/16) include a feeling of malaise (1/16) and a hypoglycemic crisis (1/16). In the patient group, 15.38% (4/26) patients treated with AVK and had morning INR values outside the ideal range (two patient had and extremely high INR and two had extremely low INR). The increased thrombotic and hemorrhagic risk in these patients led to the postponement of interventions on the advice of the treating physician.
 |
Fig. 1 Distribution according to the ASA physical status classification system. |
 |
Fig. 2 Distribution of pathologies in the population: patients with cardiovascular (n = 56), endocrine (27), neuropsychic (n = 7), orpheline (n = 13) and respiratory (n = 14) diseases. |
 |
Fig. 3 Result of observational study. |
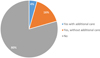 |
Fig. 4 Complication rates in study group. (Orange square) Without additional care in dental practice: patients managed in one-day-hospitalization. (Blue square) With additional care in dental practice: complication needing additional care. |
Discussion
Multiple pathologies are often the rule in the elderly [2]. The female prevalence (18.75%) of persons aged >65 years with multiple pathologies who consult dentists can be explained by higher life expectancy as well as the fact that women tend to care for their teeth more [7].
The way of evaluating treatment has been done in a pragmatic way, by leaving the treatments and interventions as they are usually practiced. The patient group, in particular, benefited from the specific strategies of at-risk patients: improving hemostasis and rinsing with tranexamic acid, in particular, for cardiovascular patients taking anticoagulants.
The rate of complications in the group of at-risk patients was statistically higher than in the control group and validates the indications that the researchers put in place in 2013. The vast majority of complications are hemorrhagic in patients with AVK confirming the increased hemorrhagic risk in elderly patients with AVK [8]. The abnormal values of INR detected on the day of the intervention, allow for a better follow-up of these patients who will be referred to their treating physicians to titrate INR values [9]. There was no need for full hospitalization, suggesting the cost-effectiveness of HDJ without posing risk to the patient, avoiding weekly hospitalization at higher cost.
Surveillance in HDJ appears to be an alternative to hospitalization, allowing the patient to return home in better circumstances [1]. This support appears particularly useful in patients with anticoagulants and/or antiplatelet agents, as the majority of complications are hemorrhagic. This strategy of HDJ is poorly developed in France when it comes to orofacial medicine but in other countries such as in Canada, where other noninvasive surgeries, such as unilateral parathyroidectomies, benefit from HDJ with proven results [5]. The interest evoked by the authors is to ensure that the patient is comfortable and can safely return home with the best resources for the minimum cost. Noninvasive acts (prosthesis, descaling) are always possible in certain cases where precautions are taken [10]. In the procedure proposed in this study, it is shown that HDJ ensures that immediate treatment is possible should perioperative complications arise and the patient can safely return home.
Following this study, a plan of action to improve the management of these patients was put in place with particular emphasis on:
closer monitoring of patients taking anticoagulants in the dentist's chair and in HDJ, who are at higher risk, in particular, by improving the guidelines available for using the tranexamic acid protocol set up in 2012 and to take account of feedback (3);
acquisition of a digital self-measuring device to check INR for patients under AVK.
Following this study, the evaluation criterion: “Rate (%) of local or general perioperative complications requiring full intervention or hospitalization of patients at risk for oral surgery with an HDJ” was proposed as a clinical practice indicator (CPI) in order to be registered in the Quality Account of the Max Fourestier institution.
These preliminary results allowed us to assess which patients required HDJ treatment at Max Fourestier Hospital. In this study, the rate of perioperative complications appears to be a relevant CPI. This study will allow researchers to follow the annual rate of these complications and allow them to adjust their actions to suit each patient at risk. In addition, this CPI will allow comparisons to be made between health facilities. Considering that no complications have resulted in complete hospitalization, HDJ has a place in the treatment protocols of oral surgery.
Conflicts of interests
The authors declare that they have no conflicts of interest in relation to this article.
Annexes
Working group
Alantar A. (Odontology, coordination), Arnaud L (Odontology), Bayet K. (Odontology), Levy-Bohbot A. (Physician), G. Fineltain (Physician, Court of Appeal expert), Gandolfini MP (Cardiology), Gellée T. (Physician), Guez P. (Quality and Risk Delegate), Levy M. (Diabetology), Maire Th (Odontology), Sabbagh R. (Resuscitation Anesthesia), Schneider P. (Nurse, HDJ), Sifi Y. (Odontology), Thangavelu A. (Odontology).
Practitioners involved
Alantar A. (Odontology-oral surgery, coordination), Arnaud L. (Odontology), Cachoire A. (Nurse, HDJ), Dame M. (Odontology-Oral Physician), Debosse B. (Medical Secretariat), Diaz R. (Odontology-oral surgery), Gandolfini MP. (Cardiology), Bayet K. (Odontology), Levy-Bohbot A. (Physician), Gellée T. (Physician), Levy M. (Diabetology), Maire Th (Odontology), Marquet M. (Assistant Caregiver), Maurice M. (Assistant Caregiver), Moudani S. (Nurse, HDJ), Orsini DP. (Odontology), Oglesby H. (Odontology), Sabbagh R. (Resuscitation Anesthesia), Schneider P. (Nurse, HDJ), Sifi Y (Odontology), Sriffine L. (Nurse, HDJ), Touboul A. (Odontology-oral surgery).
References
- HAS-ANAP. Ensemble pour le développement de la chirurgie ambulatoire. Socle de connaissances, 2012. Available from: www.has.sante.fr/portail/jcms/c_1242334/chirurgie-ambulatoire-socle-de-connaissances. [Google Scholar]
- HAS. Prendre en charge une personne âgée polypathologique en soins primaires-Mars, 2015. Available from:www.has-sante.fr/portail/docs/application/pdf/2015-04/fiche_parcours_polypathologie_du_sujet_age.pdf. [Google Scholar]
- Rapport d'EPP N°12. Référence: 46. Evaluation du risque hémorragique post extractionnel chez les patients sous clopidogrel (Plavix®) associé ou non à l'aspirine ou aux AVK, 2012. [Google Scholar]
- Recommandations. Gestion péri-opératoire des patients traités par antithrombotiques en chirurgie orale. Recommandations. Méd Buc Chir Buc 2015;2:5–14. [Google Scholar]
- Peel JK, Melck AL. Same-day discharge after unilateral parathyroidectomy is safe. Can J Surg 2016;59: 242–246. [CrossRef] [PubMed] [Google Scholar]
- Riley R, Holman C, Fletcher D. Inter-rater reliability of the ASA physical status classification in a sample of anaesthetists in Western Australia. Anaesth Intensive Care 2014;42:614–618. [PubMed] [Google Scholar]
- Vaidya V, Partha G, Karmakar M. Gender differences in utilization of preventive care services in the United States. J Womens Health (Larchmt) 2012;21:140–145. [CrossRef] [PubMed] [Google Scholar]
- Sebastian JL, Tresch DD. Use of oral anticoagulants in older patients. Drugs Aging 2000;16:409–435. [CrossRef] [PubMed] [Google Scholar]
- Recommandations pour la prise en charge des patients sous traitement anti-vitamines K en chirurgie bucco-dentaire. Société Francophone de médecine buccale et chirurgie buccale en collaboration avec la Société Française de Cardiologie. Méd Buc Chir Buc 2006;12:88–212. [Google Scholar]
- Pouysségur-Rougier V, Mahler P. Odontologie gériatrique: optimiser la prise en charge au cabinet dentaire. France: Rueil-Malmaison, Éditions CdP, 2011. [Google Scholar]
All Figures
|
Fig. 1 Distribution according to the ASA physical status classification system. |
| In the text | |
|
Fig. 2 Distribution of pathologies in the population: patients with cardiovascular (n = 56), endocrine (27), neuropsychic (n = 7), orpheline (n = 13) and respiratory (n = 14) diseases. |
| In the text | |
|
Fig. 3 Result of observational study. |
| In the text | |
|
Fig. 4 Complication rates in study group. (Orange square) Without additional care in dental practice: patients managed in one-day-hospitalization. (Blue square) With additional care in dental practice: complication needing additional care. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.