| Issue |
J Oral Med Oral Surg
Volume 32, Number 2, 2026
|
|
|---|---|---|
| Article Number | 15 | |
| Number of page(s) | 7 | |
| DOI | https://doi.org/10.1051/mbcb/2026015 | |
| Published online | 10 July 2026 | |
Original Research Article
Immunohistochemical expression of CD163, vimentin, and nerve growth factor receptor in giant cell fibroma of oral mucosa (A cross-sectional study)
1
Department of Oral Diagnostic Sciences, College of Dentistry, University of Baghdad, Baghdad, Iraq
2
Department of Oral Diagnostic Sciences, School of Dental Medicine, University Of Buffalo, New Yark, United States
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
13
May
2024
Accepted:
3
May
2026
Abstract
Objectives: Giant cell fibroma (GCF) is a rare oral mucosal lesion characterized by the presence of giant and stellate cells within its fibrous stroma. This study aimed to investigate the cellular origin and immunophenotypic profile of GCF, with particular emphasis on evaluating histiocytic and possible neural differentiation using vimentin, CD163, and nerve growth factor receptor (p75NTR). Material and methods: A total of 61 paraffin-embedded tissue sections of GCF were obtained from the archives at the College of Dentistry, University of Baghdad between 2010-2024 and stained immunohistochemically for vimentin, CD163, and p75NTR. Results: Vimentin and CD163 showed strong positivity in stromal and giant cells, with an average of 73.75% and 59.2%, respectively. However, a cytoplasmic staining of p75NTR was observed in all patients without membranous reactivity. Conclusion: The findings suggest a fibro-histiocytic origin of GCF with limited evidence of neural differentiation, which requires further investigation
Key words: giant cell / CD163 / vimentin / immunohisto-chemistry
Publisher note: The third author’s affiliation has been corrected on 23 July 2026.
© The authors, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Giant cell fibroma (GCF) is an oral soft tissue lesion with distinctive clinicopathological features [1]. Weathers and Callihan first described GCF as a separate entity among fibrous hyperplastic soft tissue lesions in 1974 when 108 out of 2000 fibrous hyperplasia specimens met the GCF criteria [2]. Unlike traumatic fibroma, GCF is not associated with chronic irritation [3].
Clinically, GCF is characterized by an asymptomatic nodular mass of <1 cm, most frequently occurring in the gingiva [4]. The surface may be smooth, lobulated, or papillary; thus, the lesion clinically appears to be a papilloma [5]. It almost always occurs before the age of 30 yr, with a slight female predilection [6]. Histologically, the surface is stratified into squamous epithelium, covering loose or dense fibrous stroma with numerous large stellate mono-, bi-, or multinucleated giant cells, well-demarcated cytoplasm, dendritic processes, and surrounded by an artifactual space or separation of collagen fibers from the cell boundaries [7].
These multinucleated giant cells are also found in other fibrous lesions such as ungual fibroma, acral angiofibroma, cutaneous giant cell fibroblastoma, and cutaneous collagenoma [8].
Despite previous discussions on GCF, the nature, phenotypic characterization, and immune profile of GCF remain elusive [9] and a few immunohistochemical studies focused on exploring the origin of the giant cells in GCF was performed since it has low incidence, prevalence, and indolent behavior [10]. Previous studies have generally pointed to a mononuclear fibroblastic origin and a fibroblastic phenotype. One cannot completely rule out the idea that some of these giant cells are derived from primitive mesenchymal tissues that may have neural or histiocytic differentiation [5–10]. Despite multiple studies, the exact cellular origin of multinucleated giant cells remains controversial. This study aims to investigate the cellular origin of multinucleated giant cells in GCF by assessing mesenchymal, histiocytic, and neural markers.
Vimentin, an intermediate filament protein, is usually associated with primitive mesenchymal malignancies [11].
NGFR (p75NTR) a transmembrane protein in the tumor necrosis factor receptor family, is widely used as a diagnostic for neural origin oral cancers, this marker was included to explore possible neural differentiation based on its expression in neural crest-derived cells [12]. CD163 a glycoprotein from the scavenger receptor cysteine-rich family, is currently the most specific marker for monocytes and macrophages in diagnostic applications due to its higher specificity compared to CD68, which may show cross-reactivity with fibroblasts [13].
Material and methods
Sample
The sample size was calculated using G power software ver. 3.1.9.7. The study power was set to 80%, alpha error probability = 0.05 (2-tailed), and correlation ρ H1 = 0.35 (moderate). The total sample size was 61 [14].
A total of 61 formalin-fixed paraffin-embedded tissue blocks of GCF, along with clinical data (age, sex, and site), were obtained from the archives of the oral pathology laboratory at the College of Dentistry, University of Baghdad, from 2010 to 2024, After obtaining approval from the ethical committee (No.004718), immunohistochemical staining was performed using vimentin, CD163, and p75NTR antibodies. The study was conducted according to SRTOBE Guidelines.
Immunohistochemistry
For the preparation of immunohistochemical analysis, serial slices of four-micron tissue sections were taken from each tissue block. The staining process was performed based on instructions provided by the manufacturer. Three primary antibodies manufactured by Abcam (Cambridge, UK) were used as an anti-vimentin antibody (ab224829), anti-CD163 antibody (ab87099), and anti-P75(NGFR) (ab227509). The antibodies were used at dilutions specified in the modified manufacturer’s datasheets.
Detection was performed using the Mouse and Rabbit Specific HRP/DAB Detection IHC kit (Abcam, ab236466; 15 ml), which was utilized for detecting all primary antibodies. Negative controls were carried out on consecutive sections with the omission of the primary antibody, resulting in no detectable staining.
All spindle and giant cells with cytoplasmic vimentin, membranous and cytoplasmic CD163, and membranous NGFR (p75NTR) expressions were considered positive based on the manufacturer data sheets of each marker.
An immunostaining assessment was performed using a light microscope (Olympus CH). All slides were initially scanned by two experienced pathologists at low power (X10) to select five representative fields, which were then visualized and scored using an X40 objective. A mean positive percentage was recorded. The percentage of positive cells was scored semi-quantitatively, as illustrated in Figure 1 and Table I.
 |
Fig. 1 A: Mean and 95% confidence interval for total immunopositive stromal cells. B: Mean and 95% confidence for the number of immunopositive giant cells. C: Vimentin correlation. D: CD163 correlation. |
Scoring system of immunohistochemical markers.
Statistical analysis
The Statistical Package for Social Sciences version 26 (IBM, USA) was used for all statistical analyses. The descriptive analysis for total immunopositive cells and positive giant cells summarized using mean, SD and 95% confidence interval. The vimentin and CD163 correlations was calculated using Pearson’s correlation test Since the data normally distributed. The significance level of p <0.05 was considered statistically significant.
Results
Expression of vimentin
Cytoplasmic vimentin expression was positive in all patients as shown in Figure 2 with a mean of 73.75% (SD = 11.91) of lesional cells and 51.08% (SD = 25.52) of giant cells and scored 4 for all patients (Figs. 1A and 1B). Despite the uniform positivity, no statistically significant correlation was identified between the proportion of total immunopositive cells and the number of positive giant cells (Fig. 1C), suggesting that vimentin expression reflects a generalized stromal characteristic rather than being specifically associated with the formation or distribution of multinucleated giant cells.
 |
Fig. 2 Immunohistochemical expression of vimentin in GCF showing strong cytoplasmic positivity in giant and surrounding spindle stromal cells. (scale bar length: 100 micron). |
Expression of CD 163
Membranous and cytoplasmic CD163 expressions were positive as shown in Figure 3 with a mean of 59.2% (SD = 12.82) of the lesional cell and 46.07% (SD = 20.27) of giant cells; however, 68.9% of patients scored 2 and 31.1% scored 1. A statistically significant positive correlation was observed between the percentage of total immunopositive cells and the number of positive giant cells for CD163 as detected in Figure 1D, suggesting that histiocytic differentiation may play a role in the formation or accumulation of multinucleated giant cells within GCF.
Furthermore, a moderate but statistically significant positive correlation was identified between vimentin and CD163 expression levels (r = 0.391, p = 0.002), supporting the concept of overlapping mesenchymal and histiocytic phenotypic features in the lesional cells.
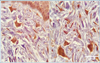 |
Fig. 3 Positive cytoplasmic and membranous expressions of the CD163 immunohistochemical marker in stromal and multinucleated giant cells of GCF. (scale bar length: 100 micron). |
Expression of NGFR (p75NTR)
In all patients, a remarkable positive cytoplasmic expression of NGFR (p75NTR) was observed, as depicted in Figure 4. Based on the manufacturer’s datasheets and previously established interpretation criteria, NGFR expression is considered positive only when membranous staining is present. Therefore, the observed cytoplasmic reactivity in this study was interpreted as negative for true neural differentiation.
This pattern may reflect non-specific cytoplasmic accumulation or intracellular sequestration of the protein rather than functional receptor expression, and thus should be interpreted with caution.
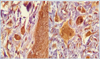 |
Fig. 4 Immunohistochemical expression of NGFR showing the cytoplasmic expression in giant and surrounding spindle cells. (scale bar length: 100 micron). |
Discussion
The assessment of the GCF immune profile in our study revealed a strong cytoplasmic positivity for vimentin. These findings align with that of previous studies suggesting a fibroblastic differentiation [9, 18–21]. However, vimentin is notably not a cell-type-specific marker for multinucleated giant cells, leaving the histogenesis of these cells elusive [20–22]. Vimentin positivity confirms the mesenchymal nature of the lesional cells; however, due to its lack of specificity, it cannot be considered definitive evidence of fibroblastic histogenesis., which is consistent with the findings of Regzie et al. [15].
The potential for histiocytic differentiation in GCF was explored by assessing the CD163 expression, a highly specific marker for histiocytic lineage differentiation (monocyte and macrophage) in the diagnostic use [17]. The specificity of CD163 was supported by the result of the study done by Lau et al., (2004) who demonstrated that CD163 is a highly specific marker for cells of monocyte/macrophage lineage, which seems suitable for routine use in paraffin-embedded tissue samples and offers an alternative to CD68 antibodies for identifying cells of monocyte/macrophage derivation in normal and neoplastic conditions [16]. The focus on macrophage-related markers in this study was intentional, as previous literature has primarily suggested a possible macrophage or fibroblastic origin of multinucleated giant cells, rather than a dendritic cell lineage.
The positive CD163 expression in all patients supports the concept proposed by Regzie et al. in 1987 [2-], whereas contradicting studies used less specific histiocytic markers such as factor XIIIa [9, 18] and CD 68 [18].
Remarkably, our study reveals a statistically significant positive correlation between vimentin and CD163 expression, suggesting overlapping phenotypic features rather than definitive evidence of histogenesis. Further, the positive correlation between the CD163 expression and the number of positive giant cells suggests a predominance of histiocytic rather than fibrous or primitive mesenchymal characteristics.
Several authors have discussed the potential neural or neuroectodermal differentiation of GCF using markers such as S-100, NSE, GFAP, and neurofilament [9, 15–19, 21].
In our study, the nerve growth factor receptor (p75NTR) was used as a more specific marker that labels both neural and epithelial structures. Intense staining of neural structures in the superficial and deep lamina propria was observed with NGFR (p75) [15]. The data sheets and prior literature on this marker in other lesions [23] reported that NGFR antibody is considered positive only when it exhibits membranous reactivity. In our study, all patients with GCF exhibited clear cytoplasmic positivity for NGFR (p75NTR). This could be due to sequestration from the membrane. The nonspecific sequestration of soluble proteins by other cells of a different lineage or the cell interstitium is a common problem in thyroglobulin detection, which can also be observed with myoglobin, glial fibrillary acidic protein, and other cellular proteins [24–26]. Although it cannot be definitively classified as positive, this finding is noteworthy and requires further validation before it can be considered as a marker for this unique lesion, however, the study of higher number of GCF cases and use of wider range of mesenchymal and histiocytic markers is recommended to improve these results.
From the clinical point of view, recent studies are supportive of a neoplastic nature of GCF rather than a reactive one, especially considering the p53 and tenascin expression, and this should implicate an autonomous but limited growth capacity of GCF. As a benign tumor [10] although fibrous overgrowths of the oral cavity are benign diseases, a histological analysis of the tissue is required to rule out the possibility of malignant alterations. These benign growths may continue to grow in size following local irritation or chronic trauma unless the source of irritation is removed, or the lesion is completely excised. Early diagnosis was required in many reported cases where the patient appeared to be of a large, unusual size and was at a higher risk of developing oral cancer, such as smokers and older age patients. Early removal of this lesion reduced the likelihood of more complex surgical intervention at a later stage [4, 27].
Acknowledging the retrospective nature of this study, our focus was narrowed to biopsy-proven GCF lesions. The relative rarity of these lesions inherently limited the scope for broader statistical analyses. It is posited that future studies, benefiting from multicenter data pooling, with inclusion of more markers such as CD68 or dendritic cell markers (e.g., DC-SIGN or CD207) could offer a more precise delineation of the pathogenesis, immunoprofile, clinical Presentation and treatment measures thus enriching the existing body of knowledge on GCF.
In conclusion, this study proved that giant cell fibroma is more favorable of fibro histiocytic origin rather than fibrous origin.
Acknowledgments
We would like to acknowledge Assistant Professor Dr. Omar mussedi for his participation and cooperation in reviewing of the study.
Special thanks to my colleagues Dr. Farah Rasheed and Dr. Noor Allawi for their assistance and support in carrying out this study.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors declare that they have no conflict of interest.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to ethical and privacy restrictions related to patient information.
Author contribution statement
Fatimah J. Ismael: Conceptualization, Methodology, Writing original draft Bashar H. abdullah: Visualization, Investigation and Supervision. Jose Luis Tapia: Writing- Reviewing and Editing.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Baghdad, College of Dentistry, Iraq (number 652622).
References
- Bhardwaj N, Bhat N, Thakur K, Dogra A. Giant cell fibroma: a case report with literature review. Int J Appl Dent Sci 2022;8:20–22. [Google Scholar]
- Weathers DR, Callihan MD. Giant-cell fibroma. Oral Surg Oral Med Oral Pathol 1974;37:374–384. [Google Scholar]
- Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology-E-Book: Elsevier Health Sciences; 2023, p. 516. [Google Scholar]
- Shetty N, Kudva A, Carnelio S, Kudva R. Giant cell fibroma of buccal mucosa-an unusual lesion of unusual size: a case report. J Oral Maxillofac Pathol 2023;27:772–775. [Google Scholar]
- Sabarinath B, Sivaramakrishnan M, Sivapathasundharam B. Giant cell fibroma: a clinicopathological study. J Oral Maxillofac Pathol 2012;16:359–362. [Google Scholar]
- Masannan Mozaffari P, Saeedi N, Mohtasham M, Khosravi F, Farjami F. Giant cell fibroma of the oral cavity: case series and literature review. J Res Dent Maxillofac Sci 2023;8:221–225. [Google Scholar]
- Kuo Y-H, Hwang M-J, Lee Y-P, Chiang C-P. Oral giant cell fibroma: a report of three cases. J Dent Sci 2021;16:552. [Google Scholar]
- de Souza IF, Salgueiro AP, Rados PV, Visioli F. Giant cell fibroma: 10-year survey in an oral pathology service. Oral Surg Oral Med Oral Pathol Oral Radiol 2020;129:e173. [Google Scholar]
- Odell E, Lock C, Lombardi T. Phenotypic characterisation of stellate and giant cells in giant cell fibroma by immunocytochemistry. J Oral Pathol Med 1994;23:284–287. [Google Scholar]
- de Oliveira IG, da Costa AAS, Meirelles DP, Tavares TS, Pinheiro JdJV, de Mesquita RA, et al. Immunohistochemical expression of p53, ki-67, tenascin, and fibronectin in giant cell fibroma and traumatic fibroma of the oral mucosa. J Oral Diagn. 2024;09:e263 [Google Scholar]
- Goswami M. Primitive myxoid mesenchymal tumor of infancy, an enigmatic entity: a case report. Indian J Pathol Microbiol 2024:67:932–935. [Google Scholar]
- Nishioka M, Aguirre RL, Ishikawa A, Nagumo K, Wang L-H, Okada N. Nerve sheath myxoma (neurothekeoma) arising in the oral cavity: histological and immunohistochemical features of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol 2009;107:e28–e33. [Google Scholar]
- Schaer DJ, Boretti FS, Hongegger A, Poehler D, Linnscheid P, Staege H, et al. Molecular cloning and characterization of the mouse CD163 homologue, a highly glucocorticoid-inducible member of the scavenger receptor cysteine-rich family. Immunogenetics 2001;53:170–177. [Google Scholar]
- Cohen J. Statistical Power for the Behavioural Sciences. Hilsdale. NY: Lawrence Erlbaum. Vil. 58, 1988, pp. 7-19. [Google Scholar]
- Regezi J, Zarbo R, Tomich C, Lloyd R, Courtney R, Crissman J. Immunoprofile of benign and malignant fibrohistiocytic tumors. J Oral Pathol Med 1987;16:260–265. [Google Scholar]
- Lau SK, Chu PG, Weiss LM. CD163: a specific marker of macrophages in paraffin-embedded tissue samples. Am J Clin Pathol 2004;122:794–801. [Google Scholar]
- Fantini F, Giannetti A, Benassi L, Cattaneo V, Magnoni C, Pincelli C. Nerve growth factor receptor and neurochemical markers in human oral mucosa: an immunohistochemical study. Dermatology 1995;190:186–191. [Google Scholar]
- Miguel MCdC, Andrade ESdS, Rocha DAP, Freitas RdA, Souza LBd. Expressão imuno-histoquímica da vimentina e do HHF-35 em fibroma de células gigantes, hiperplasia fibrosa e fibroma da mucosa oral. J Appl Oral Sci 2003;11:77–82. [Google Scholar]
- Magnusson BC, Rasmusson LG. The giant cell fibroma a review of 103 cases with immunohistochemical findings. Acta Odontol Scand 1995;53:293–296. [Google Scholar]
- Campos MS, Domaneschi C, Nunes FD, Weinfeld I. Giant cell fibroma of the maxillary gingiva in children: a case report. J Dent Child 2010;77:174–176. [Google Scholar]
- Okamura K, Ohno J, Iwahashi T, Enoki N, Taniguchi K, Yamazaki J. Giant cell fibroma of the tongue: report of a case showing unique S-100 protein and HLA-DR immunolocalization with literature review. Oral Med Pathol 2009;13:75–79. [Google Scholar]
- Kuo R-C, Wang Y-P, Chen H-M, Sun A, Liu B-Y, Kuo Y-S. Clinicopathological study of oral giant cell fibromas. J Formos Med Assoc 2009;108:725–729. [Google Scholar]
- Søland T, Brusevold I, Koppang H, Schenck K, Bryne M. Nerve growth factor receptor (p75NTR) and pattern of invasion predict poor prognosis in oral squamous cell carcinoma. Histopathology 2008;53:62–72. [Google Scholar]
- Eusebi V, Bondi A, Rosai J. Immunohistochemical localization of myoglobin in nonmuscular cells. Am J Surg Pathol 1984;8:51–56. [Google Scholar]
- Kawaoi A, Okano T, Nemoto N, Shiina Y, Shikata T. Simultaneous detection of thyroglobulin (Tg), thyroxine (T4), and Triiodothyronine (T3) in nontoxic thyroid tumors by the immunoperoxidase method. Am J Pathol 1982;108:39. [Google Scholar]
- Stanta G, Carcangiu M, Rosai J. The biochemical and immunohistochemical profile of thyroid neoplasia. Pathol Annu 1988;23:129–157. [Google Scholar]
- Oluwakuyide RT, Castano BO, Akinshipo AO, Ayodele AO. Giant cell fibroma in an elderly woman: a report of a rare, late and unusually large presentation: unusually large giant cell fibroma. Niger J Dent Res 2023;8:1–6. [Google Scholar]
Cite this article as: Ismael F.J, Abdullah B.H, Tapia J.-L. 2026. Immunohistochemical expression of CD163, vimentin, and nerve growth factor receptor in giant cell fibroma of oral mucosa (A cross-sectional study). J Oral Med Oral Surg. 32: 15. https://doi.org/10.1051/mbcb/2026015
All Tables
All Figures
|
Fig. 1 A: Mean and 95% confidence interval for total immunopositive stromal cells. B: Mean and 95% confidence for the number of immunopositive giant cells. C: Vimentin correlation. D: CD163 correlation. |
| In the text | |
|
Fig. 2 Immunohistochemical expression of vimentin in GCF showing strong cytoplasmic positivity in giant and surrounding spindle stromal cells. (scale bar length: 100 micron). |
| In the text | |
|
Fig. 3 Positive cytoplasmic and membranous expressions of the CD163 immunohistochemical marker in stromal and multinucleated giant cells of GCF. (scale bar length: 100 micron). |
| In the text | |
|
Fig. 4 Immunohistochemical expression of NGFR showing the cytoplasmic expression in giant and surrounding spindle cells. (scale bar length: 100 micron). |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.