| Issue |
J Oral Med Oral Surg
Volume 27, Number 1, 2021
|
|
|---|---|---|
| Article Number | 8 | |
| Number of page(s) | 9 | |
| DOI | https://doi.org/10.1051/mbcb/2020052 | |
| Published online | 13 November 2020 | |
Educational Article
Update on the management of orbitozygomatic fractures
1
Service de chirurgie maxillo-faciale et Stomatologie, CHU de Brazzaville, Faculté des Sciences de la Santé, Université Marien Ngouabi, Brazzaville, République du Congo
2
Service de Stomatologie et Chirurgie Maxillo-faciale, CHU d'odontostomatologie de Bamako, Université de Bamako, Bamako, Mali
3
Service de chirurgie maxillo-faciale et esthétique, CHU Mohammed VI Marrakech. Faculté de Médecine et de Pharmacie de Marrakech. Université Cadi Ayyad, Maroc
4
Service de Stomatologie et Chirurgie Maxillo-faciale, CHU de Treiche-Ville, Université Houphouët Boigny, Abidjan, Côte d'Ivoire
5
Service de Stomatologie et Chirurgie Maxillo-faciale, CHU Sourou Sanou, Université Nazi Boni, Bobo-Dioulasso, Burkina Faso
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
23
July
2019
Accepted:
26
August
2020
Abstract
Orbitozygomatic fractures are an important aspect of facial trauma. Although the literature in maxillofacial surgery is rich on the question, this article resulting from the experience of a maxillofacial surgeon brings additional data in the knowledge of the subject. This is particularly the case with regard to the principles of examination, the pathways first, the principles of restraint and osteosynthesis, and the various surgery-related complications, as well as the precautions to be adopted to minimize them. The most important thing to remember is that the management approach is often variable, and the right choice is summed up in the clinical perception and level of expertise and comfort of the surgeon, while also considering the patient's point of view.
Key words: Orbitozygomatic fractures / orbital walls / facial trauma / muscular incarceration / osteosynthesis
© The authors, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Orbitozygomatic fractures are defined as facial skeleton fractures that surround and protect the ocular globe, that is, the frontal bone, the zygomatic bone, the maxillary bone, the zygomatic process, and the temporal bone.
These fractures account for approximately 10–25% of all facial fractures. They are quite commonplace for young men and are mainly caused by public road accidents and violent attacks [1].
Mastering the characteristic features of these fractures is essential to manage them appropriately as well as to avoid and significantly reduce their esthetic and functional side effects.
Although some basic principles are being included in the literature nowadays, the practical modalities and indications for selection are yet to be discussed.
Thus, the purpose of this work, which has been written in the form of a pedagogical article, is to share the managerial vision of a maxillofacial surgical team concerning orbitozygomatic fractures and to successively address its general features, aspects of the examination, its clinical management, as well as possible side effects.
Background
Understanding the basic orbitoocular anatomy and the radioclinical characteristics of lesions is necessary to ensure proper patient care.
Reviewing the orbital surgical and anatomopathological anatomy
The orbit is shaped like a pyramidal cone with its base in the anterior portion and its peak in the posterior; the most anterior part of its walls or orbital rim is formed by the thick cortical bone, which provides stable support, or the craniofacial skeleton. The middle third of these walls is significantly thinner and more prone to rupture [1].
Each wall varies in thickness and thus the thinnest walls, namely the medial wall and the floor, are the most vulnerable.
The medial wall
The medial orbital wall has four structural and functional characteristics [2]:
-
First of all, this part of the orbit separates the orbital content from the ethmoid cells, which explains the occurrence of orbital emphysema when it fractures.
-
Second, the internal wall and its rim constitute an insertion site for the inner canthal tendon. Inner wall fractures can, therefore, lead to telecanthus and canthal dystopia.
-
Third, the anterior and posterior clusters of the inner canthal tendon envelope the lacrimal sac. Serious damages to this wall may result in a lacrimal sac lesion.
-
Finally, the anterior and posterior ethmoid arteries cross the internal wall at the point where it joins the orbital roof, transporting blood from the ophthalmic artery to the nasal cavity. Although the ethmoid arteries may be small in size, damage to these vessels can cause significant intra-orbital hemorrhage or even an orbital syndrome.
Inner wall fractures must, therefore, be meticulously evaluated because of their potential effects on these associated structures.
The floor
Although the inner wall is thinner, a back-to-back effect created by the ethmoid lamellae makes it easier to fracture the orbital floor than the medial wall. The fragility of the floor results in a higher occurrence of fractures, especially due to bursting “blow out” and greenstick or “trapdoor” fractures that trap the lower right muscle, which is common in children.
Although muscular incarcerations occur more frequently in the posteromedial part due to the close apposition of the muscles and their respective orbital walls, incarceration can nonetheless occur before or behind the orbit, which could limit ocular motility and possibly cause double vision more frequently in the posterior incarcerations [3,4].
It must be noted, however, that there is no direct relationship between double vision and the incarceration of an oculomotor muscle. Back et al. have shown that 80% of the patients who initially experienced motility problems displayed spontaneous healing in the shortest time possible [5]; this is explained by possible damage to the orbital soft tissue (nerve paresis, lower right muscle contusion, and a local edema) without incarcerations.
However, limited ocular motility along the vertical or horizontal axis is very indicative of a dysfunctional oculomotor muscle, hence the importance of conducting a forced duction test and CT scan (transverse and coronal sections).
The lateral wall
The thick lateral wall, on the other hand, is also supported by the temporal muscle, which protects against both medial and lateral displacement, causing the lateral wall to fracture less frequently, unless these fractures are linked to those of the zygomatic arch or maxillary [6].
The roof of the orbit
Roof fractures are frequent among the pediatric population experiencing pneumatization of the craniofacial skeleton and rare in adults because of the thickness of the bone and the proximity of the frontal sinus, which may collapse and eliminate the impact.
Its onset in adults is often directly caused by violent craniofacial impact.
Consequently, these fractures are often linked to the presence of a neurologic lesion in 57–90% of cases, ocular damage in 14–38% of cases, damage of the other orbital walls in 76% of cases, and in 33% of cases to other facial fractures [7].
Furthermore, because of the proximity of the upper right muscle and upper oblique muscles, there is a risk of associated incarceration.
As with all the orbital fractures, there is the risk of exothalmia and enophthalmos based on the direction of displacement of the fractured bone fragments. The association with neurologic lesions involves a greater risk of meningitis and would probably require a neurosurgical consultation, even though 80% of these lesions heal spontaneously and can be strictly managed with intravenous antibiotics, not forgetting the possibility of an anti-pneumococcal vaccine [8].
The exam
The initial evaluation
As with any maxillofacial trauma, an appropriate evaluation must obey the rules respecting what constitutes a prioritized emergency. Certainly, in the emergency department, maxillofacial lesions are often forced to take a back seat compared to other so-called vital emergencies, but an evaluation is necessary to rule out functional emergencies.
Indeed, prolonged exposure of the cornea, for example, may result in microbial keratitis.
The key elements of the physical examination must be based on a three-stage symmetrical inspection of the face, eye, and appendices, using a penlight.
Meticulous periorbital palpation in search of any exquisite tenderness, “step-off” sign, and subcutaneous crackling must be performed.
The ocular motricity exam and the evaluation of intraocular pressure can be done quickly by asking the patient to open their eyes. The easy and complete opening of the eyelid generally excludes acute orbital pressure [1,3].
Should the patient fail to cooperate, assessing the intraocular pressure can be done by gently parting the upper and lower eyelids with a finger.
In the event of elevated orbital pressure, the globe rests against the eyelids, thereby creating a resistance to opening the eyelid.
Visual acuity, the visual fields, checking the pupil, the dilated eye exam with a direct ophthalmoscope, and a cranial nerve exam must all be included in the analysis.
The clinical signs most often observed in adults are periorbital ecchymoses and subconjunctival hemorrhage (Fig. 1).
Even in the absence of perceptible, physical signs, some patient's complaints should attract the attention of practitioners and cause them to strongly suspect an orbital fracture, including such signs as exophthalmia (though minimal), palpebral edemas, intraorbital pressure, palpebral or periorbital crackling, limitation of ocular motility, swelling of the cheeks, nasal deformation, ocular pains and nausea at the time of ocular motility, ptosis, an unexplainable desire to keep one eye closed after trauma, and limited buccal opening. All these signs associated with understanding the mechanism and the type of accident should cause them to suspect an orbitozygomatic fracture.
However, the absence of signs does not necessarily exclude a fracture, especially in children who often present with floor fractures without any microscopic signs, referred to as “white-eye fractures.” They are often revealed by an isolated ocular motility disorder.
Furthermore, 5% of adults who have experienced cranial trauma have undiagnosed orbitozygomatic fractures and about half of them require surgery [9].
All these lesional presumptions must be certified by performing a craniofacial CT scan on bony fenestrations, axial, coronal and sagittal sections and three-dimensional reconstruction. This makes it possible to identify the bone lesions, their characteristics, and to detect the presence or absence of neurologic and or ophthalmologic lesions.
 |
Fig. 1 Periorbital ecchymoses. |
The ophthalmologic exam
Considering the significant risk of intraorbital lesions, it is reasonable that all patients suspected of having an orbital fracture would benefit from a complete and formal ophthalmologic exam to rule out less severe lesions and allow practitioners to care for the orbitozygomatic fractures. However, it is also incumbent on all maxillofacial surgeons to conduct a proper evaluation of the ocular and periocular lesions because they are responsible for the patient's recovery.
Orbitozygomatic fractures are associated with 11–15% of ophthalmologic emergencies, some examples of which are a sudden decline in visual acuity or other visual problems [10].
However, it is important to note that declines in visual acuity are not always caused by an ophthalmologic emergency because eyelid edemas, for example, can cause a temporary but significant false decline in visual acuity.
The majority of ophthalmologic emergencies linked to an orbitozygomatic fracture are often secondary to the orbital syndrome. This syndrome can be caused by acute hemorrhaging (most often indicating suborbital arterial lacerations or posterior ethmoid arteries), a soft tissue edema, an orbital crash causing impaction of the intraorbital bone tissue, orbital emphysema due to damage to the adjacent sinuses, an orbital fat incarceration, creating a sudden intraorbital pressure. It can cause direct ocular harm or even cut into or compress the optic nerve.
In children, the determination of ocular motility disorder can be difficult. This type of injury must therefore be feared when the child presents with an orbital fracture, with associated nausea and vomiting because this clinical triad is usually predictive of motility disorders in more than 80% of the cases. This requires a rigorous exam with a CT scan to confirm the incarceration of the lower right muscle [11].
It must be noted that animal studies have shown an irreversible vision loss after about 90 min of tissue hypoxia [10]. Every minute can count; thus, it will be imprudent for a surgeon to be the first to highlight such lesions and to wait for an ophthalmologic consultation rather than to act immediately.
Orbital syndrome with the optical nerve compression test is an extreme emergency and requires orbital decompression either by conducting open surgery or by guided needle aspiration by CT scan or even lateral cantholysis. If lateral cantholysis is the selected option, know that profound, orbital pressure will ensue, rapid hemorrhage can lead to progressive exophthalmia, whose expansion is not stopped by the effect of the eyelids, and in rare cases, elongation or even avulsion of the optical nerve may result.
Other ocular lesions found in 0.5% of the orbital traumas [12] can constitute emergencies but are less extreme, especially, they can be in the form of a rupture of the ocular globe, lacrimal damage, retinal detachment, vitreous hemorrhage, hyphema, a lesion of the oculomotor muscles, bone fragments impinging on the globe orbital cellulite and a traumatic neuropathy of the optical nerve.
Traumatic optical neuropathy may be caused by direct damage to the nerve by the following: a penetrating object, broken bone fragments impinging on the nerve, transmission of vibration forces of the craniofacial skeleton toward the optical nerve with or without facial fracture, the shearing force in the optical foramen, or by one extrinsic nerve compression (hematoma) or intrinsic (hematoma or edema).
A strong suspicion for this type of lesion must be evoked for all orbitozygomatic traumas, which present with contusions at the occipital level, on the glabella, or on the superolateral orbital rim, changes in visual acuity, visual field reduction, and an abnormal pupillary response.
The radiological exam
The most useful imaging modality in patients with trauma is the creation of axial, coronal, and sagittal sections for an orbitozygomatic CT scan. Generally, the cuts must be 3 mm, but in situations where less details are necessary, cuts of 1.25 mm or less are suitable [1,3,5]. Three-dimensional reconstruction (3D) is not always necessary for isolated orbital fractures.
Coronal sections are particularly useful for orbital roof and floor fractures to identify damage to the oculomotor muscles, as well as to assess the degree of enophthalmia and exophthalmia.
Axial cuts are predictive of medial wall fractures.
Finally, sagittal cuts can be useful to evaluate orbital roof and floor fractures, but they are also indicated for postoperative auto-evaluation, which is dear to the young surgeon.
However, it must be noted that there is still no correlation between CT imaging and the clinical elements, because, someone may have muscular incarcerations on the scan, for example, without any ocular motility disorder. Some blatant muscular incarcerations may go unnoticed by the CT scan.
In terms of the exam, we adopt the Zingg classification as a reference for fracture of the zygoma [13].
– Category A: Partial or isolated fracture of one of the three processes of the zygomatic bone:
-
The temporal process (A1) forming the zygomatic arch.
-
The frontal process (A2) forming the lateral, orbital rim.
-
The maxillary process (A3) forming the infraorbital edge.
– Category B: Fracture-disjunction of the zygomatic bone with rupture of the four attachments.
When displaced, it is often in:
-
rotation with a pivot avec pivot inside.
-
Impaction in the maxillary sinus (luxation below, within, and behind) often associated with an orbital floor fracture. Thus, influencing the direction of reduction, which must be opposite to the direction of displacement.
-
Valgisation, very rare.
– Category C: comminuted fracture linking a zygomatic crash with Category B lesions.
– Category D: fracture isolate from the body.
How soon to commence care
Care can be immediate or deffered. The length of time varies according to schools, but a general average is 7–14 days after experiencing trauma, before soft tissue scarring begins, and after all the swelling has disappeared.
Past 2 weeks, soft tissue fibrosis and a callus of fibrous bone, particularly in young subjects, may appear, hence the importance of making provisions for the curettage of fibrous tissue [3].
Surgical techniques
Patient care depends on the type of fracture, ranging from the percutaneous reduction using Dingman's or Ginestet's hook to a reduction of bleeding with osteosynthesis.
The purpose of the treatment is to reduce the fracture and, consequently, the deformation in order to restore ocular and masticatory functions.
The surgical indication in the orbitozygomatic fractures depends on the morpho-functional impact including the modification of the volume within the orbital cavity.
First, the path chosen will depend not only on the habits of the operator but also and especially on the expected benefits to be gained from the therapeutic strategy. They must first think before choosing the intervention about how they intend to access the given anatomical area, the amount of exposure that will be obtained, the authorization of the surgical operation, and the esthetic outcome.
Reducing the orbitozygomatic fracture site has three main objectives: restoring the force lies of massive bones, preserve ocular function, and reestablish the orbital volume.
An intravenous bolus of corticoids must be administered before the intervention to reduce edema before operating, which can distort the estimations of the position of the globe and increase the risk of postoperative orbital congestion with possible vision damage.
The orbital roof
Non-displaced orbital roof fractures are often managed conservatively.
Fractures displaced upwards may require intracranial pressure monitoring. However, if there is an associated neurologic lesion which requires an intervention, the fracture can be repaired at the same time by accessing the cranium.
Fractures displaced downwards can cause exophthalmia and should be treated surgically.
Other surgical indications are initiated in cases of double vision, a restricted gaze, lagophthalmia, linked to either a cranial nerve lesion, incarceration of the upper oblique muscle, upper right, and problems lifting the upper eyelid.
Roof fractures can be approached by making an upper blepharoplasty incision, indicated in the ablation of a bone fragment. The best approaches for its osteosynthesis remain the coronal and transcranial approaches (Fig. 2).
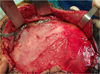 |
Fig. 2 Multifocal roof fracture, associated with a fracture of the zygomatic arch, treated by osteosynthesis via coronal access. |
The orbital floor
The most common indication for the urgent repair of an orbital floor fracture is the incarceration of an oculomotor muscle. Two types of floor fractures can be identified: “pure” floor fractures (no damage to infraorbital margin) and “impure” fractures (with damage to the infraorbital margin).
The non-urgent surgical indications for orbital floor fractures include fractures that affect more than 50% of the floor (Fig. 3), substance loss greater than 1 cm2, enophthalmia upwards of 2 mm, and persistent double vision.
The surgical exploration of the orbital floor is necessary for any fracture with a displacement of at least 1 cm.
Exploration of the posterior part of the orbit is advised after a reduction of the zygomaticomaxillary complex (ZMC) to increase the likelihood of muscular incarceration post-reduction.
The orbital floor approaches are divided into transcutaneous and transconjunctival approaches.
The main transcutaneous approaches (infraciliary, medial palpebral, and inferior palpebral) are adapted to provide a wider exposure of the orbital floor but result in an external scar [14].
The infraciliary approach significantly improves the risk of postoperative ectropion.
Nonetheless, this remains the most frequently chosen approach. Among the other remaining transcutaneous approaches, the medial palpebral is better than the inferior orbital approach because of its esthetic results, particularly in older patients with well-defined subtarsal wrinkles.
The transconjunctival approach exposes the orbital floor without any external scarring and also limits postoperative ectropion when performed via the retroseptal route [15]; however, when a greater exposure is necessary, this approach is often complemented by a lateral canthotomy.
The transconjunctival and medial palpebral approaches via the retroseptal route seem to be the safest options to avoid any postoperative complications.
 |
Fig. 3 “Impure” floor fracture with more than 50% substance loss from the floor, medial palpebral approach used. |
The medial wall
Indications for the repair of the inner wall are essentially, the incarceration of right, medial muscle with clinical repercussions and substance loss resulting in enophthalmia, often rare, because of the force of gravity which does not ordinarily displace the intraorbital content in the adjacent nose and ethmoid.
The inner wall approaches are: Lynch's transcutaneous approach, the transconjunctival and the transnasal incision. The Z-plasty modified Lynch incision, involves an incision starting in the inferomedial part of the forehead at the naso-jugal junction 5 mm away from the medial canthus.
Different areas of the conjunctiva can be used as a point of departure to access the inner wall. The transcaruncular or retrocaruncular incision gives access to the area by an incision through or posterior to the caruncle and anterior to the semilunar fold. This eliminates the external scar. However, the access provided by this approach is not satisfactory and can prove difficult for more complex fractures. Some precautions must also be taken to avoid scarring between the globe and the eyelids.
An inferior transconjunctival approach can also be used with or without upward medical extension, but special care should be taken to avoid damaging the lacrimal drainage system and insertion of the superior oblique muscle. For extended fractures, (the nasoorbitoethmoid fractures and orbital roof fractures), access can be gained via a bicoronal approach.
The lateral wall
Fractures of the external orbital wall, which require surgical intervention are generally linked to fractures of the zygomatic bone, also known as the ZMC, or tripod zygomatic fractures, and most often result in a lateral point of impact on the cheek. If the bone fragments are not reduced, persistent flattening and widening of the affected side of the face will ensue, the lateral canthus tendon may be displaced, and the globe may be mispositioned. If the orbital volume is reduced, the patient may have exophthalmia, but if the orbital volume is increased, this can indicate enophthalmia.
The lateral orbital wall can be exposed using several examples [3,13,15]:
-
A lateral incision, or an incision into the tail of the eyebrow.
-
A transconjunctival incision above the lateral canthus paying close attention to the levator muscle inside the eyelid and the lacrimal gland. This incision facilitates access to the supero-external wall.
The hemicoronal approach can also be used.
Constraints and reconstruction
The constraint of a fracture, by definition, comes into play, after the reduction. It brings together different methods aimed at stabilizing this reduction with the overarching goal of obtaining consolidation.
Consolidation of a stable fracture site, that has been correctly reduced, ordinarily occurs at the facial skeletal level within six weeks. Pseudarthroses are rare. They are most often secondary to a false indication in the use of constraint methods or of a reinfection.
Several methods are used from the simplest to the most complex [3,15].
Steel wire
Steel wire ligatures achieve excellent cooptation of the fractured fragments, but excessive stranding can modify the reduction performed whereas insufficient stranding does not ensure proper and sufficient constraint and can be a source of pseudoarthrosis.
In any event, supple 3/10 wire is used as a monocortical ligature to bring together and coopt the small fragments, like the size you would find in the infraorbital margin; 4/10 and 5/10 steel wires are used for monocortical ligatures in areas where the bone is densest and thickest (frontozygomatic apophyses).
The orifices where the steel wire is introduced must be made with at least a semi-long strand adapted to match the gauge of the required wire. The advantage presented by steel wire ligatures is that the constraint can be achieved without removing the periosteal of the bone fragments. Preserving the periosteal is one of the key elements of the proper fracture consolidation.
Plates
Arciform microplates made of titanium between 0.6 and 1.6 mm thick are used.
Kirchner transfacial pins
The transfacial pins are only used for constraint or to support osteosynthesis by mini plates for the lateral wall fracture or the zygomatic disjunction fracture (Fig. 4).
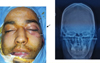 |
Fig. 4 Frontozygomatic constraint using a transfacial Kirchner pin (image of patient on the operating table to the left and that of the postoperative follow-up to the right). |
Screws
Titanium screws are chosen, varying in size from 1.2 to 2 mm, features include: a head, a reverse angle, a diameter, a tip and threading most likely thread forming.
Techniques for the placement of plates and screws
The fracture site is approached from beneath the periosteal, curetted and reduced, a microplate of the size that best matches the fracture is chosen. Two or three holes must be made on either side of the fracture site, the closest screws are placed at least 2 mm away. The plate must be modelled to conform to the curve of the bone on either side of the fracture site. Once the modeling of the plate has been completed, it is attached using an operator by distributing the holes of the screws on either side of the fracture. The screws must imperatively be positioned on an abutment or periorbital spacer so that the cortical thickness will be sufficient to obtain the proper primary hold. The first screw to be put in place will be the one nearest to the fracture site of the most stable fractured bone at the level of its most stable fragment. The screw is placed following slow monocortical drilling under continuous irrigation to avoid heating up the bone because that will cause bone necrosis along the screw thread and compromise the final hold of the screw (and thus the stability of the mount).
The size of the drill bit used is slightly inferior to that of the threaded screw thread to allow for auto-thread forming.
The drilling axis is important, it determines the screwing axis. This is done for “perfect” reductions with neutral screwing, only exerting a pure axial pressure regulated by the tightening force, the drilling/screwing axis must be centered in the middle of the hole on the plate. Maximal angulation of 15 to 20° allows the material to conserve the pure, axial compression force. The screw is then placed in the drilled hole. Screwing must be done slowly to allow for auto-thread forming. The tightening of the first screw must not be at maximal force from the outset. One to two screws are placed on the same fragment, screwing must be rigorously neutral, at this point the initial tightening pressure is at maximum and the first screw is properly secured.
However, in cases of a “less perfect” reduction, two methods of drilling/screwing allow you to imprint a constraint by compressing the site of the fracture with a classical system.
-
a drilling-screwing axis perpendicular to the bone and the plate whose point of application is off-center in the plate hole, this point can maintain a maximum distance from the fracture site. While screwing the reverse angle buts prematurely against the plate and imprints a recentering movement of the screw inside the plate hole, which consequently exerts a compression force on the fracture site. Inversely, if the point of application is off-center in the direction of the fracture site, a distraction force is applied on the fracture site.
-
a drilling-screwing axis angled in relation to the bone and plate and diverging from the fracture site. The phenomenon is identical. However, an angle of more than 20° between the drilling/screwing axis and the plate/bone is formally discouraged. It disrupts the distribution of constraints and exposes the patient to an increased risk of secondary destabilization.
Other screws are inserted neutrally.
Reconstruction methods
Reconstructing the orbital walls is often necessary. There are two major options for reconstructing the substances lost from the orbital walls: autologous grafts and alloplastic implants.
For the autologous grafts, there are:
-
The bone graft, harvested from the cranial vault, iliac crest, ribs, or fibula.
-
The cartilaginous graft harvested from the auricle (Fig. 5), iliac bone, or rib.
The disadvantages of these types of grafts are the potential morbidity of the donor site, irregular graft contours, and graft resorption.
For the alloplastic implants, there are:
-
The titanium grill, porous, high-density polyethylene, and many other materials that can be used as bone substitutes. They are relatively inert, a reliable support is assured without donor site morbidity, and they adapt easily to the contour of the orbit.
Furthermore, the majority of orbital floor implants on non-smooth surfaces do not require fixation because of the nature of their surrounding structures and their relative immobilization.
The reconstruction of orbital trauma in children is a particular process and must obey certain principles. Small fractures can be treated with resorbable bio-prostheses, such as polylactic polymers and polymers in polyglycolic acid. With their resorption properties over the period of one year, such materials do not seem to limit skeletal growth as with rigid fixations.
At the end of the orbital fracture reconstruction, a forced duction test must be done to ensure the complete freedom of the globe.
During the reconstruction, the surgeon must ensure optic nerve integrity by the proper positioning of the materials, which must not be placed too far back to avoid any traumatic, optic neuropathy.
 |
Fig. 5 Reconstruction of the floor from an auricular graft in the patient on the left. Harvesting site of auricular cartilage by retro-auricular access in the patient on the right. |
Surgical outcomes
Simple outcomes
Postoperation, two elements must be kept in mind [1,3,5,7,15,16]:
-
the protection of the cornea and,
-
avoiding optic nerve compression.
Several management possibilities make it possible to protect the cornea: lubricating, ophthalmic ointments, Vaseline, clear adhesive dressings, and the use of Frost or blepharorraphic sutures of short duration, because closing the eyelids contributes to decreased visual acuity and no longer allows the orbit to decompress because of ptosis that is aggravated by orbital edema, thus resulting in orbital syndrome.
The use of lubricating ointments or a transparent, adhesive dressing reduces this risk.
Pain and nausea management are essential to reduce the risk of increased pressure in the orbital vein in addition to postoperative intraorbital hemorrhage.
Visual acuity and ocular motility tests in patients are done systematically after surgery at 2-h intervals for 48 h.
Complications
Several complications have been described [15,16]:
-
Optic neuropathy secondary to contact with implants or reconstruction materials;
-
Orbital hemorrhaging or edem, which is the most severe complication;
-
Muscular damage, which cannot be easily managed secondarily, even with strabismus surgery;
-
The most common complications are enophthalmia and ectropion.
When enophthalmia occurs suddenly after orbital reconstruction, it is most often secondary to insufficient intraorbital volume due to incorrect positioning of materials or an improper fracture reduction. When it occurs progressively, on the other hand, it is often due to atrophy of the orbital muscle fat.
In both cases, a CT scan must be conducted to assess the orbital volume and determine whether it is the implant or the materials that have been incorrectly positioned.
Mispositioning is corrected by repositioning the implant in its correct anatomical position. In the case of progressive enophthalmia, the orbital volume can be reestablished with alloplasties or autogenous bone grafts.
Orbital floor fracture and infraorbital margin
Ectropion is the main complication. It can be caused either by improper healing, laxism of the lateral canthus tendon, and/or excessive tension during anterior repair by the excessive excision of the tissues.
It can be avoided with a meticulous surgical approach, Frost's suture, canthopexy, and canthoplasty.
Most cases can be resolved by massaging the lower eyelids and by forced eye closure exercises. Surgical indication must be reserved for those patients with corneal exposure.
Postoperative double vision also counts among the complications and must be subject to exploration by CT scan to exclude the incarceration of the inferior right muscle after reconstruction.
Delayed liberation of incarcerated muscle exposes the patient to the increased risk of ischemia and muscular fibrosis which in turn limit ocular motility and cause double vision.
Even after the timely liberation of the incarcerated inferior right muscle, a patient may have originally had double vision and now develop postoperative hyperopia because of the weakness of the muscle. In children, this resolves spontaneously over the 9 months. In adults, strabismus surgery is usually required.
Orbital cellulite is also a complication that develops in 0.8% of cases according to patients' risk factors, such as nasal sinusitis at the time of the trauma or when excessively blowing one's nose [15]. However, antibiotic prophylaxis reduces the incidence of orbital cellulite in the immediate post-traumatic period and is generally reserved in case of coexistence with sinusitis, especially if associated with the administration of corticoids [17].
Fracture and the medial wall
The most significant complications to look out for are optic nerve damage and lesions of the right medial muscle with limited ocular motility. The other potential complications are essentially the telecanthus, a lesion or obstruction of the lacrimal pathways and double vision. Minor disorders of horizontal motility are more readily tolerated than those of vertical dysmotility.
Lateral wall fracture
Complications associated with the lateral wall are essentially linked to the lack of fracture reduction and fixation. Adequate repositioning of the lateral wall plays a vital role in determining the orbital volume, because its fractures tend to displace the entire orbitozygomatic complex, which causes a huge increase in the orbital volume thereby affecting the positioning of the ocular globe.
Ectropion is also possible if the damaged lateral canthus is not repaired.
Roof fracture
As always, the most noteworthy postoperative ocular complication of orbital surgery is blindness, which may develop subsequent very strong pressures exerted on the globe or optic nerve. Delayed orbital roof fracture complications are mainly linked to the proximity of the intercranial cavity and frontal sinus. They are, encephalocele, mucocele, and osteomeningeal breach. Other complications associated with orbital roof repair are hematomas, infections, incision-dissection related damages to the eyebrow arch or the supratrochlear nerves, and some lesions of the levator muscle in the eyelid.
Conclusion
The management of orbital fractures is delicate, mainly because of the variability of lesions, the proximity of the eyes and the brain, and the position that the eyes and orbits occupy as a focal point in the middle of the face.
Particular attention must be paid to the preoperative assessment of lesions, to having an individualized surgical plan, to the honest appreciation of its actual limits and to using a rigorous surgical technique based on mastering the anatomy in order to reduce as far as possible, the functional and unesthetic sequalae.
The majority of functional and unesthetic sequalae associated with trauma and surgery are optic neuropathy, ectropion, ocular motility disorders, ocular lesion, or the unsightly appearance. These sequalae require delicate repair considering the uncertainty of the results.
Conflicts of interests
None.
References
- Duhamel P, Giraud O, Denhez F, Cantaloube D. Facial trauma exam. EMC Elsevier Masson SAS, Paris), Stomatologie, 22-068-A-05, 2002. [Google Scholar]
- Ferré JC, Chevalier C, Helary JL, Le Cloarec AY, Legoux R, Le Tenneur J, et al. Craniofacial bone biomechanics. EMC (Elsevier Masson SAS, Paris), Stomatologie, 22-001-D-15, 1995. [Google Scholar]
- Wirth C, Bouletreau P. Trauma surgery of the facial skeleton .EMC (Elsevier Masson SAS, Paris), Techniques chirurgicales-Chirurgie plastique reconstructrice et esthétique, 45-505-B, 2011. [Google Scholar]
- Soparkar CNS, Patrinely JR. The eye examination in facial trauma for the plastic surgeon. Plast Reconstr Surg 2007;120:49S–56S. [Google Scholar]
- Back CPN, McLean NR, Anderson PJ, David DJ. The conservative management of facial fractures: indications and outcomes. J Plast Reconstr Aesthet Surg 2007;60:146–151. [Google Scholar]
- Barbrel P, Géré E. Orbital fractures. EMC (Elsevier Masson SAS, Paris), Stomatologie, 22-072-A-10, 2001. [Google Scholar]
- Fulcher TP, Sullivan TJ. Orbital roof fractures: management of ophthalmic complications. Ophthal Plast Reconstr Surg 2003;19: 359–363. [CrossRef] [Google Scholar]
- Raaf J. Posttraumatic cerebrospinal fluid leaks. Arch Surg 1967; 95:648–651. [Google Scholar]
- Exadaktylos AK, Sclabas GM, Smolka K, et al. The value of computed tomographic scanning in the diagnosis and management of orbital fractures associated with head trauma: a prospective, consecutive study at a level I trauma center. J Trauma 2005;58:336-341. [CrossRef] [PubMed] [Google Scholar]
- Mellema PA, Dewan MA, Lee MS, Smith SD, Harrison AR. Incidence of ocular injury in visually asymptomatic orbital fractures. Ophthal Plast Reconstr Surg 2009;25:306–308. [CrossRef] [Google Scholar]
- Lane K, Penne RB, Bilyk JR. Evaluation and management of pediatric orbital fractures in a primary care setting. Orbit 2007;26:183–191. [CrossRef] [PubMed] [Google Scholar]
- Steinsapir KD, Goldberg RA. Traumatic optic neuropathy. Surv Ophthalmol 1994;38:487–518. [CrossRef] [PubMed] [Google Scholar]
- Zingg M, Chowdhury K, Ladrach K, Vuillemin T, Sutter F, Raveh J. Treatment of 813 zygoma-lateral orbital complex fractures. New aspects. Arch Otolaryngol Head Neck Surg 1991;117:611–620. [CrossRef] [PubMed] [Google Scholar]
- Richard L, Bouletreau P, Cantaloube D, Delay E. Incisions and sutures in maxillofacial surgery and Stomatology. EMC (Elsevier Masson SAS, Paris), Stomatologie, 22-325-A-10, 1998. [Google Scholar]
- Meyer C, Groos N, Sabatier H, Wilk A. Séquelles à long terme des fractures du plancher de l'orbite operées. A propos d'une serie de 242 patients. Rev Stomatol Chir Maxillofac 1998;99:149–154. [Google Scholar]
- Merville LC, Real JP. Dislocation fronto-orbito-nasales. Initial total reconstruction. Tactique. Avantages. Servitudes. Ann Chir Plast 1979;33:488–490. [Google Scholar]
- Westfall CT, S hore JW. Isolated fractures of the orbital floor: risk of infection and the role of antibiotic prophylaxis. Ophthalmic Surg 1991;22:409–411. [Google Scholar]
All Figures
|
Fig. 1 Periorbital ecchymoses. |
| In the text | |
|
Fig. 2 Multifocal roof fracture, associated with a fracture of the zygomatic arch, treated by osteosynthesis via coronal access. |
| In the text | |
|
Fig. 3 “Impure” floor fracture with more than 50% substance loss from the floor, medial palpebral approach used. |
| In the text | |
|
Fig. 4 Frontozygomatic constraint using a transfacial Kirchner pin (image of patient on the operating table to the left and that of the postoperative follow-up to the right). |
| In the text | |
|
Fig. 5 Reconstruction of the floor from an auricular graft in the patient on the left. Harvesting site of auricular cartilage by retro-auricular access in the patient on the right. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.