| Issue |
J Oral Med Oral Surg
Volume 25, Number 1, 2019
|
|
|---|---|---|
| Article Number | 4 | |
| Number of page(s) | 5 | |
| Section | Cas clinique / Short case report | |
| DOI | https://doi.org/10.1051/mbcb/2018032 | |
| Published online | 22 February 2019 | |
Short Case Report
Gangrenous cervicofacial cellulitis from odontogenic infection: two clinical cases
Centre Hospitalier Universitaire de Dijon, Dijon, Bourgogne France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
14
August
2017
Accepted:
19
August
2018
Abstract
Introduction: Cervicofacial cellulitis resulting from common odontogenic infections is rare but serious, with life-threatening complications and potential general or local complications. Observation: Two cases are discussed here. The first observed case concerned a 32-year-old patient, affected by gangrenous cellulitis, following the avulsion of teeth number 38. The second observed case was of a chronic periapical infection being left untreated. The urgency of these two cases required the coordination of medical and surgical specialist teams to ensure a stable and successful treatment, involving surgical treatment, drug therapy, and reanimation. Discussion: The inadequate treatment or chronic dental infections, associated with immunosuppression and some cofactors (tobacco, alcohol, drugs, pregnancy, etc.), can lead to severe case of cellulitis. Medical and surgical management should be carried out as soon as possible to prevent the onset of serious complications such as mediastinitis, septic shock, and thrombophlebitis.
Key words: cellulitis / surgery / emergency treatment / focal infection / dental / complications
© The authors, 2019
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Gangrenous cervicofacial cellulitis is a cellulo-adipose tissue disorder of the face and neck related to a dental infection. It accounts for 24% of admissions to emergency departments [1]. Thus, odontogenic cellulitis is one of the primary emergencies in dentistry that can lead to worst prognosis. Diffuse gangrenous cellulitis develops from polymicrobial flora where anaerobic flora predominates. It is characterized by the extensive and rapid necrosis of cellular tissues, with a risk of septic shock. It is an absolute medical and surgical emergency [2]. The clinical and biological signs of an infection are often visible. The main contributing factors are an immunocompromised state, diabetes, and the use of non steroidal anti-inflammatory drugs (often associated with a delayed patient consultation) [3,4].
Case 1
A 32-year-old patient presented to the emergency department of the Center Hospitalier de Montbard (located 80 km north-east of Dijon) for a left submandibular swelling with a significant alteration from the normal state, which was followed by the extraction of teeth number 18, 28, and 38 performed under general anesthesia on an outpatient basis 4 days previously. The patient was prescribed an antibiotic (roxithromycin; Rulid®), analgesic (paracetamol/dextropropoxyphene; Propofan®), and a nonsteroidal anti-inflammatory drug (ketoprofen; Profenid®). He was then transferred to the emergency department at the University Hospital Center (UHC) in Dijon. An interview did not reveal any particular medical or surgical history; in addition, the patient was not a smoker, and his oral condition was healthy. His general condition was significantly altered and was rapidly deteriorating: hyperthermia at 39.8 °C and chills were noted. Biologically, he had an inflammatory syndrome with a CRP level of 232.5 mg/L. Extraoral examination showed large, left submandibular swelling, which was erythematous and painful on palpation, was associated with severe trismus, and was without dysphagia. The pain score was assessed as 9 on the visual analog scale. The patient was treated by emergency physicians, admitted to the hospital, and was sent the next day for an orthodontic consultation, with an intravenous prescription of amoxicillin/clavulanic acid, metronidazole, paracetamol, and tramadol.
Clinical examination showed a rapid and unfavorable evolution with bilateral and cervical extension of the swelling as well as a large increase in its volume (Fig. 1). The palpation was painful and crackling.
Orthopantomogram was immediately performed (Fig. 2) in addition to cervical contrast-enhanced computed tomography (Fig. 3), which revealed the scale and severity of gangrenous cellulitis with purulent and laterocervical bilateral necrotic collections.
Next, the patient was treated in the operating room under general anesthesia by the Oto-Rhino-Laryngology Department of the University Hospital of Dijon for drainage of the purulent collection and excision of necrotic chambers via cervicotomy (Fig. 4). Drainage shunts were placed, and the operative site was sutured (Fig. 5). The patient was intubated using a fiberscope.
The patient was then transferred to the surgical intensive care unit for further management. He was febrile at 40 °C postoperatively. An intravenous probabilistic antibiotic therapy [cefotaxime (Claforan®) and metronidazole (Flagyl®)] was administered while awaiting the results of bacteriological analysis. He had a biological inflammatory syndrome with CRP levels of 300 mg/L, procalcitonin levels of 50 µg/L, and a decrease in leukocyte count from 17.4 to 8.9 g/L. He was transferred the next day to the Edouard Herriot Hospital in Lyon for possible treatment with hyperbaric oxygen therapy (which could not be implemented) with the following: cefotaxime, gentamicin, esomeprazole, metronidazole, fentanyl, midazo lam, norepinephrine, enoxaparin sodium and paracetamol (in case of fever).
He was hospitalized again at Dijon UHC 3 days later with the aim of improving his condition over the next 14 days. Different samples collected during the first intervention showed the presence of group F streptococcus, which was sensitive to penicillin G. Therefore, antibiotic treatment was readministered, and the patient was started on amoxicillin and metronidazole. The evolution was favorable; the patient was afebrile and was discharged after 14 days of hospitalization with continued antibiotic therapy for 10 days and daily dressing until the area had healed completely.
The patient was followed up after 10 days and showed a remarkable clinical improvement despite an unsightly scar for which he was prescribed a protective skin cream (Madecassol®) and physiotherapy sessions for cervical drainage and given photoprotection instructions. He was reviewed after 3 months with a favorable clinical assessment. Biannual oral examination was prescribed at the attending oral surgeon's clinic.
 |
Fig. 1 Bilateral cervical swelling with local signs of intense inflammation. |
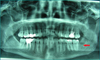 |
Fig. 2 Panoramic radiograph. |
 |
Fig. 3 Cervical CT scan with radiocontrast agents. |
 |
Fig. 4 Cervicotomy with purulent discharge and presence of necrotic tissue. |
 |
Fig. 5 Immediate postoperative situation. |
Case 2
A 68-year-old patient presented to the emergency department at the Auxerre Hospital Center for acute dental pain in the third quadrant, which had been increasing for 3 days. He had taken self-medication with nonsteroidal anti-inflammatory drugs (ibuprofen, 400 mg). The pain was accompanied by progressive onset of edema, dyspnea, odynophagia, and a significant change in the general condition due to which he was transferred to the emergency department of Dijon UHC for specialized care. Examination revealed obliterating arteriopathy of the lower limbs and chronic obstructive pulmonary disease in a chronic alcohol-smoking context, combined with the absence of medical and dental follow-up for many years. Extraoral clinical examination revealed diffuse, poorly circumscribed, erythematous, and acutely painful left and cervical submandibular swelling on palpation. Intraoral clinical examination revealed a poor overall oral condition, with only 7 teeth remaining on the arch: 11, 12, 23, 37, 38 (impacted), 43, and 44, without any prosthetic rehabilitation. The patient was hemodynamically stable, and cervicofacial contrast-enhanced CT showed large diffuse gangrenous cervicofacial cellulitis (Fig. 6). The patient was then treated in the emergency room under general anesthesia by the maxillofacial surgery department at the Dijon UHC for the drainage of the purulent collection, extraction of teeth numbers 43, 44, and 37, establishment of Delbet® drainage shunts, and closure of the operative site. The surgical procedure was complicated postoperatively by respiratory distress following post-extubation laryngeal edema, which was treated by emergency reintubation. The patient was then transferred to the multipurpose intensive care unit for further management and postoperative monitoring. Probabilistic antibiotic therapy with Augmentin® was administered (6 g per day in three doses, intravenously). The patient's progress in the intensive care unit was marked by several instances of hemodynamically rapid atrial fibrillation requiring several chemical cardioversions with amiodarone. From a respiratory perspective, several negative leak tests contraindicated extubation and confirmed the diagnosis of postoperative laryngeal edema. Finally, at the renal level, postoperative acute functional renal failure was present in remission after several vascular filling sessions. The deterioration of the clinical state during hospitalization was attributed to the occurrence of large laryngeal edema, pus in the oral cavity, and extension of the initial purulent collection, which required cervicotomy and tracheostomy as well as amended antibiotic treatment with amikacin, Tazocillin® (piperacillin and tazobactam), and intravenous metronidazole. The prognosis was subsequently favorable, and the patient was shifted to the multidisciplinary surgical unit after 7 days. Based on the analysis of bacteriological specimens in the operating room, antibiotic treatment was revised according to the recommendations of the Infectious Diseases Department: ceftazidime administered through electric syringe pumps, ciprofloxacin (400 mg, three times a day), and metronidazole (500 mg, three times daily) administered intravenously. However, QT prolongation on ECG required early discontinuation of ciprofloxacin. The patient was back in the operating room 10 days after the initial surgery for drainage and lavage of the cervicotomy site, changing of the tracheostomy cannula, and placement of a nasogastric tube. Sudden arterial hemorrhage at the cervicotomy site required a third surgical procedure for restoring hemostasis under general anesthesia 16 days postoperatively. The prognosis was subsequently very favorable, with weaning of the tracheostomy, and the patient was finally discharged 25 days after hospitalization. Table 1 illustrates the treatment timeline of the patient during hospitalization. Local homecare for tracheostomy opening and cervicotomy scar was provided by a nurse, and regular clinical checks in the maxillofacial surgery department were performed, with a favorable prognosis. Consultation with a dental surgeon was necessary for general prosthetic rehabilitation with the extraction of the remaining non-conservable teeth (11, 12, and 23) and making of complete maxillary and mandibular removable prostheses.
 |
Fig. 6 Cervicofacial CT scan with evidence of the collection. |
Therapeutic chronology (surgicsal procédures, hospitalization, antibiotic therapy).
Discussion
Diffuse cellulitis is a sudden, severe disease with major general and regional repercussions that can lead to death in one third of the cases [1]. Many serious systemic complications have been described, which include mediastinitis [5], whose prognosis is particularly unfavorable, with 44% of deaths [6]; septic shock with visceral involvement (hepatic, renal, gastrointestinal, and respiratory); and craniofacial thrombophlebitis [7,8]. Its origin is often dental or periodontal in nature (pericoronitis, periapical infection, and periodontal abscess) but can also be related to an infection of the main salivary glands or ENT area (e.g., sinusitis maxillary, and otitis).
From its initial origin, the infection tends to spread in various deep anatomical chambers, which are compartmentalized by cervicofacial fascias and fibrous or aponeurotic lamina, which can limit its infectious spread. Its propagation can take place directly through any “weak areas” (diffusion of cellulitis), by necrosis of fascia (necrotizing fasciitis), or indirectly through septic thrombophlebitis. Additional radiographic examinations, especially cervicofacial CT, are essential for the management of this severe form of cellulitis. In fact, imaging modalities enable precise, three-dimensional observation of the extent of infection according to different anatomical chambers, suspected complications (in particular, diffusion to the endocranial and mediastino-pulmonary spaces), and surgical planning [9]. However, it is worth noting that radiological assessment is important but should not delay emergency treatment in severe cases (including necrotizing fasciitis).
From an epidemiological point of view, the 2007 study by Rakotoarison et al. [10] showed an increase in the number of cases of cervicofacial cellulitis due to the misuse of drugs, especially in cases of self-medication with uncontrolled anti-inflammatory drugs and antibiotics. Nonsteroidal anti-inflammatory drug abuse is found in more than half of the cases (up to 80%) according to the study by Bennani-Baïta et al. [11]. Among the subjects most affected by diffuse cellulitis are men aged between 20 and 30 years, patients with poor oral hygiene, and those belonging to poor socioeconomic classes. Cofactors such as older age; underlying systemic disease; the consumption of alcohol, tobacco, or drugs; nutritional imbalance; diabetes; and pregnancy have also been reported in some studies [12–15].
Conclusions
The management of diffuse cervicofacial cellulitis should be performed as early as possible. Hospitalization is inevitable, and the coordination of various medical and surgical teams is essential to ensure that the three aspects of treatment, including medical (with massive broad-spectrum intravenous antibiotics), surgical (cervicotomy to ensure the drainage of the purulent collections and removal of any necrotic tissue, possible thoracotomy in case of mediastinal diffusion), and intensive care (depending on the patient's general condition; may require intubation or tracheotomy because of dyspnea), are taken care of. Notably, this is a severe and potentially fatal infection, which can be prevented with proper oral hygiene and provision of dietary hygiene education to the patients.
Conflicts of interests
The authors declare that they have no conflicts of interest in relation to this article.
References
- Ahossi V, Perrot G, Thery L, Potard G, Perrin D. Urgences odontologiques, EMC Elsevier Masson SAS Paris Médecine D'urgence 25-170–10 (n.d.), 2007. [Google Scholar]
- Ragot JP. Stomatites infectieuses, Encycl Méd Chir Elsevier Paris AKOS Encycl. Prat. Médecine 4-1010 (n.d.). [Google Scholar]
- Bouletreau P, Froget N, Gleizal A, Breton P. Affections du plancher de la bouche, EMC Elsevier Masson SAS Paris Médecine Buccale 28-285-V-10 (2008). DOI:10.1016/S0000-0000(08)53242-6. [Google Scholar]
- Souillard-Scemama R, Dubrulle F. Pathologie inflammatoire et infectieuse de la sphère oto-rhino-laryngologique. EMC Radiol Imag Médicale Musculosquelettique Neurol Maxillofac 31-675–10. 7 (2012) 1–16. [Google Scholar]
- Dubernard C, Bellanger S, Chambon G, Herve L, Torres JH, Lozza J. Cellulite d'origine dentaire engageant le pronostic vital: à propos d'un cas. Med Buccale Chir Buccale 2009;15:119–125. DOI:10.1051/mbcb/2009010. [CrossRef] [Google Scholar]
- Garatea-Crelgo J, Gay-Escoda C. Mediastinitis from odontogenic infection. Report of three cases and review of the literature. Int J Oral Maxillofac Surg 1991;20:65–68. [CrossRef] [PubMed] [Google Scholar]
- Verma R, Junewar V, Singh RK, Ram H, Pal US. Bilateral cavernous sinus thrombosis and facial palsy as complications of dental abscess. Natl J Maxillofac Surg 2013;4:252–255. DOI:10.4103/0975-5950.127664 [CrossRef] [PubMed] [Google Scholar]
- Dagain A, Thiéry G, Dulou R, Delmas JM, Pernot P. Thrombophlébites craniofaciales, EMC Elsevier Masson SAS Paris Médecine Buccale 28-355-B-10 (2008). DOI:10.1016/S0000-0000(08)53272-4 [Google Scholar]
- Cassagneau P, Varoquaux A, Moulin G. Exploration radiologique des infections cervico-faciales. J Radiol 2011;92:1015–1028. DOI:10.1016/j.jradio.2011.08.006 [CrossRef] [PubMed] [Google Scholar]
- Rakotoarison R, Ramarozatovo N, Rakoto F, Rakotovao F. Cellulites cervico-faciales: à propos de 41 cas, Med Buccale Chir Buccale 2008;14:35–39. DOI:10.1051/mbcb/2008012 [CrossRef] [EDP Sciences] [Google Scholar]
- Bennani-Baïti AA, Benbouzid A, Essakalli-Hossyni L. Cervicofacial cellulitis: the impact of non-steroidal anti-inflammatory drugs. A study of 70 cases. Eur Ann Otorhinolaryngol Head Neck Dis 2015;132:181–184. DOI:10.1016/j.anorl.2015.06.004 [CrossRef] [PubMed] [Google Scholar]
- Bali RK, Sharma P, Gaba S, Kaur A, Ghanghas P. A review of complications of odontogenic infections. Natl J Maxillofac Surg 2015;6:136–143. DOI:10.4103/0975-5950.183867 [CrossRef] [PubMed] [Google Scholar]
- Ko H-H, Chien W-C, Lin Y-H, Chung C-H, Cheng S-J. Examining the correlation between diabetes and odontogenic infection: A nationwide, retrospective, matched-cohort study in Taiwan. PLoS ONE 2017;12:e0178941. DOI:10.1371/journal.pone.0178941 [CrossRef] [PubMed] [Google Scholar]
- Huang L, Jiang B, Cai X, Zhang W, Qian W, Li Y et al. Multi-Space Infections in the Head and Neck: Do Underlying Systemic Diseases Have a Predictive Role in Life-Threatening Complications? J Oral Maxillofac Surg 2015;73:1320.e1–1320.e10. DOI:10.1016/j.joms.2015.04.002 [Google Scholar]
- Doumbia-Singare K, Timbo SK, Keita M, Mohamed A, Guindo B, Soumaoro S. Cervico-facial cellulitis during pregnancy: about a series of 10 cases in Mali. Bull Soc Pathol Exot 2014;107:312–316. DOI:10.1007/s13149-014-0401-6 [CrossRef] [PubMed] [Google Scholar]
All Tables
Therapeutic chronology (surgicsal procédures, hospitalization, antibiotic therapy).
All Figures
|
Fig. 1 Bilateral cervical swelling with local signs of intense inflammation. |
| In the text | |
|
Fig. 2 Panoramic radiograph. |
| In the text | |
|
Fig. 3 Cervical CT scan with radiocontrast agents. |
| In the text | |
|
Fig. 4 Cervicotomy with purulent discharge and presence of necrotic tissue. |
| In the text | |
|
Fig. 5 Immediate postoperative situation. |
| In the text | |
|
Fig. 6 Cervicofacial CT scan with evidence of the collection. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.