| Issue |
J Oral Med Oral Surg
Volume 27, Number 4, 2021
|
|
|---|---|---|
| Article Number | 47 | |
| Number of page(s) | 10 | |
| DOI | https://doi.org/10.1051/mbcb/2021035 | |
| Published online | 15 October 2021 | |
Original Research Article
Jaw osteonecrosis in patients treated with denosumab 120 mg with regular dental monitoring: 4-year retrospective study
1
Dental Care Center in Rennes University Hospital, 2 rue Henri Le Guilloux, 35000 Rennes, France
2
Pharmacovigilance, Pharmacoepidemiology and Drug Information Center, Rennes University Hospital, Rennes, France
3
Centre Eugène Marquis, Avenue de la Bataille Flandres-Dunkerque, 35000 Rennes, France
4
Clinique La Sagesse, Rennes, France
5
Univ Rennes, CHU Rennes, REPERES [Pharmacoepidemiology and Heath Services Research] − EA 7449, 35000 Rennes, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
9
May
2021
Accepted:
11
September
2021
Abstract
Background: Medication-related osteonecrosis of the jaw (MRONJ) is an expected, but rare adverse effect of denosumab. There are few data denosumab 120 mg related MRONJ occurrence when regular dental monitoring is planned. International and French recommendations do not detail the schedule of the follow-up visits, allowing local interpretations. Methods: The aim of this retrospective study was to describe our local experience of regular dental monitoring in patients receiving denosumab 120 mg. We included all ≥18-year-old patients exposed to denosumab 120 mg, bisphosphonate- and denosumab-naive, and with regular dental monitoring (pre-treatment and every 4 months after denosumab initiation) at the University Hospital Center, France, from 2015 to 2019. The crude incidence of denosumab-related osteonecrosis of the jaw was estimated per 100 person-years (95% confidence interval). Results: During the study period, 251 patients were included, of whom 77 did not attend the 1st follow-up visit at 4 months. Almost all patients had osteonecrosis of the jaw risk factors. Ten MRONJ cases were reported (four stage 0 and six stage 1). The crude incidence rate was 5.1 per 100 person-years (95% CI: 1.9–8.2). Denosumab was stopped in all patients who developed MRONJ, with favorable outcome for 3 cases and stabilization in 4 cases after osteonecrosis of the jaw management. Conclusion: This study suggested that a regular dental follow-up every 4 months may be a suitable option for prevention and early detection/treatment of MRONJ. A randomized study should be performed to determine the best dental monitoring schedule.
Key words: Denosumab / osteonecrosis of the jaw / dental monitoring
© The authors, 2021
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Bone metastases are major and frequent skeletal complications in many cancers, and they are associated with considerable pain, increased mortality, and reduced quality of life (QoL) [1–3]. Antiresorptive drugs, such as bisphosphonates at high doses (zoledronate acid, ibandronic acid, and pamidronate acid) and denosumab 120 mg (antibody against receptor activator of nuclear factor kappa-B ligand, RANKL), are used to reduce the risk of skeletal complications in adults with advanced malignancies. Due to its higher efficacy in preventing cancer-related skeletal complications [3–8], denosumab has been gradually supplanting bisphosphonates, and the indication for denosumab 120 mg might be expanded [9–12].
Medication-related osteonecrosis of the jaw (MRONJ) is the main, but rare, expected adverse effect of antiresorptive drugs [13], with a severe impact on physical and mental health (e.g., pain, eating difficulties, reduced social contacts), and it is hard to treat [14]. More than 90% of MRONJ cases are observed in patients with cancer receiving high doses of zoledronate acid or denosumab 120 mg [15]. MRONJ pathogenesis is not fully elucidated, and considering the well-known MRONJ risk factors [6,16–19] (cumulative exposure to antiresorptive drugs, dental extraction, denture wearing, etc.), dentists have an important role in reducing MRONJ risk. As the pharmacological mechanisms of bisphosphonates and denosumab are different [3,4], specificities in the pathogenesis of denosumab-related MRONJ cannot be excluded.
The American association of oral and maxillofacial surgeons (AAOMS) in 2014 and the European Society for Medical Oncology recommend in their updated guidelines a dental checkup and when feasible, complete invasive dental treatments before initiating therapies with bone-targeted agents. However, they do not give any information on dental monitoring after denosumab initiation [20,21]. In France, whereas the French National Health Agency (ANSM) recommends an every 4 months dental monitoring for patients receiving bisphosphonates [22], there is no information on follow-up visits for patients on 120 mg denosumab [23,24].
To date, the impact of preventive measures on MRONJ occurrence has been assessed in patients receiving bisphosphonate or denosumab, without differentiating between treatments [25,26]. Moreover, data are limited on regular dental monitoring in patients exposed to denosumab 120 mg, and practices seem to be heterogeneous [27,28]. To improve the knowledge about practices for MRONJ prevention/early detection, the aim of our study was to describe our experience of regular dental monitoring of patients exposed to denosumab 120 mg at the Dental Care Center of an University Hospital Center in France. We estimated the crude incidence rate of denosumab related-MRONJ, and described MRONJ stages and the time to disease onset.
Materials and methods
Study design and setting
This was a retrospective cohort study based on the medical and dental records of patients referred by their oncologist or a specialist physician for a dental examination before denosumab initiation and who were followed up at the Dental Care Center of a single French University Hospital Center between September 10, 2015 and September 26, 2019. The study focused on patients with regular dental monitoring.
Inclusion and exclusion criteria
Only adult patients (≥18 years) treated with denosumab 120 mg (irrespective of the therapeutic scheme) with regular dental monitoring at the Dental Care Center were included. Patients who refused to participate, received bisphosphonates or denosumab for osteoporosis before the prophylactic dental measures (visit before starting denosumab 120 mg) or had a history of radiation in the maxillofacial area were excluded. Patients who agreed to receive denosumab 120 mg, to be followed as explained in the regular dental follow-up protocol (see below) of who were not dead, lost to follow-up or did not missed the prophylactic dental care before the drug start were included in the analysis.
Drug exposure
According to the summary of the product characteristics, denosumab 120 mg is injected once every 4 weeks. The monthly injection was performed at the patient's home by a nurse. The date of the first denosumab injection was considered as the follow-up start date (T0). The duration of drug exposure was estimated by taking into account the cumulative number of injections and five half-lives after the last injection.
Regular dental monitoring protocol
Before starting denosumab 120 mg for any indication, the following preventive dental measures were implemented: (i) thorough dental assessment, including dental radiography, dental panoramic radiographs, and periapical radiographs or cone beam computed tomography of selected teeth, if needed; (ii) complete information about the risk of MRONJ and oral hygiene advices; (iii) presence of dental plaque, an indicator of oral hygiene, using the Silness-Löe plaque index (PI): no plaque (PI = 0), film of plaque visible in situ after application of disclosing solution or by probing the tooth surface (PI = 1), moderate accumulation of soft matter (PI = 2), abundant soft matter (PI = 3); (iv) dentures were examined to assess their fitting and the absence of any compression area and/or pressure ulcers. Patients were reminded about the importance of not wearing their dentures for approximately 8–12 hours per day, at least during the night; (v) non-restorable teeth were extracted. Only when extraction was needed, denosumab injection was delayed until the mucosa has healed and adequate bone remodeling has occurred, between 90 and 120 days, confirmed by a radiographic control. The post-dental extraction radiographic control that confirms bone healing after extraction was implemented from October 2016.
Then, follow-up visits were scheduled every 4 months during and up to 4 months after the end of denosumab treatment. A panoramic radiograph was performed at the pre-treatment dental assessment and every 8 months during the follow-up visits (after denosumab start). Panoramic radiograph was mostly used for prevention purposes, and cone beam computed tomography for diagnostic purposes in patients in whom MRONJ development or dental infection was suspected.
After starting denosumab 120 mg, invasive dental procedures were contraindicated, when possible. In the event of dental infections that could not be controlled without extraction, elective dentoalveolar surgery was carried out at the Dental Care Center after stopping denosumab treatment for 5 to 9 months to take into account the drug half-life (temporization period). Indeed, a washout period equivalent to five half-lives of denosumab is required to fully eliminate the molecule. Extractions were performed under antibiotic prophylaxis (amoxicillin with clavulanic acid, or clindamycin with metronidazole in cases of allergies), in an atraumatic manner, and by smoothening the sharp bony edges and with thorough mucosal wound closure using fibrin sealant. Fibrin sealant was preferred due to its high concentration of fibrinogen and thrombin that significantly hasten the formation of a fibrin meshwork and protect the surgical site from oral contaminants. Antibiotic treatment was continued until complete mucosa healing (amoxicillin with clavulanic acid, or clindamycin with metronidazole in cases of allergies). This schedule was extrapolated from the ANSM guidelines to prevent bisphosphonate-related ONJ [22].
If MRONJ was detected, denosumab was stopped, and a conservative management was put in place during the period of decreasing effectiveness of the antiresorptive drug. This approach included rigorous oral hygiene, antibacterial mouthwashes, systemic antibiotic therapy in the case of superinfection, and not wearing overlying dentures. MRONJ surgical management was planned 5–9 months after denosumab withdrawal, depending on the exposure duration. Approximately 6 months after denosumab interruption, bone sequestration may appear spontaneously, as well as bone remodeling. Surgery was then performed by a senior surgeon (RG and SCL), mostly under general anesthesia, followed by 5-day hospitalization with a gastric probe. On the basis of our experience, a specific surgical approach was used: (1) high full-thickness mucoperiosteal flap to reveal the entire area of exposed bone; (2) extended resection of the affected bone to reach healthy-looking and bleeding bone; (3) sharp edge smoothing; (4) primary soft tissue closure with fibrin sealant and appropriate mucosal or local muscle flap. Antibiotics were administered from the day before and for at least 21 days after the intervention. Mucosa healing and bone remodeling on radiograph were monitored at week 5 and month 3 after surgery (healing period), respectively. Denosumab re-introduction was discussed on a case-by-case basis.
Outcome
The outcome was denosumab-related MRONJ occurrence after treatment start. MRONJ diagnosis was confirmed by a senior dental surgeon during a follow-up visit at the Dental Care Center. MRONJ diagnosis and staging were based on the 2014 AAOMS updated criteria (Tab. I) [20].
Staging proposed by the American Association of Oral and Maxillofacial Surgeons (AAOMS).
Data collection and statistical analysis
Demographic and clinical variables were considered: sex, age at the pre-denosumab dental assessment, primary cancer type, current cancer treatments (e.g., chemotherapy, glucocorticoids, anti-angiogenic drugs), dental MRONJ-precipitating factors (periodontal disease, removable dentures, implants, dental extraction), MRONJ stage. Data were summarized using descriptive statistics (i.e., mean and frequency).
The follow-up duration was estimated from denosumab start to: the patient death, MRONJ diagnosis during exposure to denosumab (the date of the follow-up visits at which MRONJ diagnosis was made), the date of the last follow-up visit for patients without MRONJ and still receiving denosumab, the date of treatment stop plus five half-lives, or the study period end, whichever occurred first. In the absence of information on the exact number of injections between follow-up visits (4 months), an arbitrary average number of 2 injections was considered.
The crude MRONJ incidence rate was estimated by dividing the number of denosumab-related MRONJ cases by the cumulative denosumab exposure duration of all patients (from denosumab initiation to the date of the follow-up visit at which MRONJ was detected during treatment, or if no MRONJ was detected, the date of the last follow-up visit when the patient was still exposed or the date of treatment stop), and expressed in person-years with the 95% confidence interval (95% CI). Crude analysis was also estimated by excluding patients who did not attend the first 4-month follow-up visit. For descriptive purposes, the Kaplan-Meier method was used to estimate the event (MRONJ)-free survival (EFS) rate by taking into account interval-censored data. Indeed, the exact moment at which the MRONJ occurred was unknown, although it occurred at some point between the date of the last visit without MRONJ and the date of the first visit with MRONJ (4 months). EFS was estimated using the nonparametric maximum likelihood estimator (NPMLE) and the survival curve data with the EM-ICM algorithm available in the ICLIFETEST procedure (SAS version 14.1).
Ethical aspect
Ethical approval was granted by the University Hospital research ethic committee (#19.140). Informed consent was obtained from each patient.
Results
Between 2015 and 2019, 352 patients underwent a prophylactic dental examination before denosumab initiation at the University Hospital Center. Finally, on the basis of the inclusion and exclusion criteria, 251 patients (73% of women) were selected for this study (Fig. 1). MRONJ risk factors were detected in 214 patients (85%) and MRONJ-precipitating dental factors in 158 patients (63%). It should be noted that 12 patients who had dental extractions started denosumab only after mucosal healing, without bone remodeling achievement control (since the radiographic control was put in place in our protocol later). Two patients with lung cancer started denosumab despite the presence of chronic oral infections at the prophylactic visit, due to the treatment urgency. The patients' baseline characteristics are described in Table II and the results of the pre-treatment dental assessment in Table III. After denosumab start, all patients received one injection monthly, except five patients with giant cell tumor who received four injections in the first month, followed by one injection monthly, and two patients who received two injections in the first four months (instead of four) followed by one injection monthly. Moreover, for the 33 patients who died close to the 4-month visit, 13 patients who were lost to follow up before 4 months (8.8% of patients), and 31 patients who did not reach 4 months of treatment (due to administrative censoring), it was arbitrarily considered that they received two denosumab injections in total. At the study end, 25 patients had completed the treatment (10 to 30 injections; duration of denosumab treatment was decided by the oncologist).
During the follow-up, five patients (2%) presented dental pathologies (after 7 to 12 injections) that required extraction of the causal tooth. None of these patients developed secondary bone events during the period of denosumab withdrawal for dental pathology treatment. Three patients could restart treatment after alveolar bone healing without any new oral event during the rest of the follow-up (3 injections for two, and 8 injections for one patient).
Among the 251 patients, 10 MRONJ cases were observed that were classified as stage 0 or 1 (Tab. IV). Figure 2 shows the distribution of patients with and without MRONJ according to the denosumab exposure duration. The crude MRONJ incidence rates were 4.5/100 person-year (95% CI: 1.7–7.3) for the whole population, and 5.1/100 patient-year (95% CI: 1.9–8.2) when excluding the 77 patients who did not attended the first 4-month follow-up visit. The MRONJ-free survival rate was >80% at 24 months (Kaplan-Meier survival curve in Fig. 3). All MRONJ cases were reported to the Pharmacovigilance Regional Center at the University Hospital Center. Denosumab was stopped in all patients with MRONJ, without any skeletal-related event. Regarding the outcome of the MRONJ, resolution was observed in one case, improvement in two (during post-surgical healing period), stabilization in four cases (observed during the temporization period), and one case worsened after surgery on the affected tooth; two patients died during the temporization period. Only one patient (patient #1) started again denosumab 6 months after surgery for MRONJ and bone healing control, without MRONJ recurrence after 4 months of denosumab treatment, suggestive of a complete MRONJ resolution. MRONJ risk factors were identified in all 10 patients who developed MRONJ (Tab. IV). Specifically, periodontal disease, which concerned almost 25% (n = 60) of the cohort, was observed in 90% of patients with MRONJ, and acute episodes of periodontitis (local infection) in three of them (patients #5, #7, #8). Among the 12 patients who started denosumab without bone remodeling achievement after tooth extraction, two developed MRONJ (patients #1 and #2) in the unhealed post-extraction socket. Among the 72 patients with dentures, 6 developed MRONJ, and denture compression was considered to be a precipitating factor in 5 of them. Concerning the 2 patients with lung cancer and oral infection who started denosumab in emergency, one did not show any dental problem during the follow-up (7 injections), while the second was lost to follow-up before 4 months.
 |
Fig. 1 Study flowchart. |
Patients' baseline characteristics.
Baseline oral characteristics.
Description of the patients with MRONJ.
 |
Fig. 2 Number of cases of MRONJ in function of denosumab exposure duration (number of injections). |
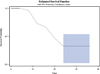 |
Fig. 3 Estimated MRONJ-free survival. Times in months. |
Discussion
MRONJ incidence rate and early detection
Between 2015 and 2019, at the Dental Care Center of a single University Hospital Center in France, among the 251 patients with regular dental follow-up before and during denosumab treatment (every 4 months), 10 cases of MRONJ were diagnosed. Excluding the 77 patients who did not attended the first 4-month follow-up visit, the crude incidence rate of 5.1/100 patient-years (95% CI: 1.9–8.2). Only MRONJ stages 0 or 1 were observed, between 8 and 24 months after denosumab start. The delays are consistent with American and Japanese studies that reported MRONJ appearance after a median number of 11.5 denosumab injections, and a median time of 10 months after denosumab start, respectively [25,27].
According to the AAOMS and literature data, between 0.7 and 11.4% of patients treated with denosumab 120 mg for cancer will develop MRONJ [5,7,15,18,20,25–29]. Most of these studies did not take into account the implementation of dental preventive measures. Variability in MRONJ incidence could be related to methodological choices, for instance, excluding patients with dental risk factors of MRONJ or pooling all the drugs. Several studies did not provide information on MRONJ stage, and the others mainly reported stage 1 to 3. A recent QoL analysis in patients with MRONJ suggested that higher MRONJ stage is associated with worse QoL, with the most marked difference between stage 1 and 2 [14].
Since 2010s, international recommendations to prevent MRONJ in patients receiving bone-targeting agents or denosumab 120 mg advocate a systematic dental check-up before treatment initiation, but do not give precise information on follow-up visits after denosumab initiation [20–23]. This has led to heterogeneous practices around the world. In a recent French retrospective study in the Loraine region that identified nine cases of MRONJ among 141 patients treated with denosumab 120 mg, regular dental monitoring (follow-up visit once per month for 6 months) concerned only 25.5% of patients [28]. An American study suggested the preventive role of regular dental check-ups in MRONJ, based on their 10-year experience in a cancer center in New York, USA, with a follow-up every 3 months for the first 2 years and biannually thereafter, without information on drugs and MRONJ stages [25]. A Japanese study also emphasized the value of regular dental monitoring, despite the fact that nearly 50% of the diagnosed MRONJ cases were stage 3 and the implementation of oral check-up visits before denosumab initiation and every month thereafter [27]. This finding could be explained by a less complete dental monitoring protocol (not described in the Japanese study) than the one carried out in our center.
MRONJ risk factors
Dental extractions, periodontal disease, dentures, chemotherapy and anti-angiogenic therapy are known MRONJ risk factors [6,18,19]. They concerned almost 85% of patients in our cohort and all patients with MRONJ.
Socket bone remodeling after tooth extraction is recommended before denosumab initiation to minimize the MRONJ risk. Previous studies proposed a delay of 14–21 days (i.e., just after mucosal healing) [25,27,28]. In our local experience, while we used this delay initially (12 patients concerned), we modified our dental monitoring protocol in late 2016 to extend the delay at 90 days (except for patients with therapeutic emergency for whom delay was reduced) with routine radiological confirmation of bone healing, as suggested in a recent review by Nicolatou-Galitis et al. in 2019 [6].
It should be noted that the presence of MRONJ risk factors and MRONJ occurrence in one patient of our cohort did not contra-indicate denosumab restart after MRONJ management. A previous study described MRONJ occurence 13 months after denosumab 120 mg initiation in a patient who was previously treated with zoledronic acid and had periodontal disease and tooth extraction [30]. Bone sequestration was observed 9 months after denosumab withdrawal and the drug was reintroduced 11 months after discontinuation, without bone exposure at the MRONJ sites. In the summary of product characteristics for Xgeva® (denosumab 120 mg), MRONJ occurrence is not identified as a contraindication to its reintroduction, and is not mentioned by ANSM [22].
Study strengths
First, the originality of our study is the individual and preventive management of patients treated with denosumab 120 mg by monitoring dental risk factors of MRONJ before and during the follow-up, according to a standardized protocol used by all dental surgeons at the Dental Care Center.
Second, to limit confusion due to drug indication heterogeneity and immortal time bias, we included only patients who never used denosumab and without history of/or current treatment with bisphosphonates or with lower doses (60 mg) of denosumab.
Study weaknesses
First, a selection bias could exist since patients could have been referred elsewhere than the Dental Care Center. But because this is a referral center for performing dental monitoring, especially in cancer patients exposed to antiresorptive drugs, we assume the number of patients who were referred elsewhere is marginal.
Second, considering the observational and retrospective design of our study, data could be incomplete or missing, and the patient follow-up limited to the medical records of our Dental Care Center. But we assume that MRONJs are preferentially managed in our Dental Care Center rather in general dental practitioners.
Third, the precise date of MRONJ onset could not be determined because the diagnosis was made during the follow-up visits at the Dental Care Center. Thus, the time to MRONJ onset was potentially overestimated. However, the regular dental follow-up every 4 months for all patients of our cohort partially reduced this bias. To take into account this point, we performed an EFS estimation with interval-censored data. The short follow-up and early death (a competitive event in MRONJ detection) before the first follow-up visit of some patients also limited the possibility of MRONJ detection. Nevertheless, the low percentage of patients lost to follow-up (8.8%) demons-tration the importance of this regular check-up that should be integrated in the management of these patients.
Four, the diagnosis of stage 0 MRONJ was introduced only in 2018. Therefore, some previous stage 1 MRONJ cases might have been diagnosed later than their real onset time. It is interesting to note that the only two MRONJ cases detected before 2018 were diagnosed at stage 1.
Finally, considering that MRONJ is a rare event, the small size of our study population, with only ten MRONJ cases observed, is an important limitation. Therefore, we did not have the statistical power to reliably estimate the risk of MRONJ in patients receiving denosumab 120mg, or to assess the impact of potential risk factors.
Overall, considering the heterogeneity of dental monitoring (frequency and type of check-up), the impact of MRONJ stage on the patients' QoL and the limitations of our retrospective observational study, it is now important to perform a multicenter randomized controlled trial to determine the best dental monitoring schedule to prevent MRONJ. A cost-effectiveness study could be also be interesting. To best of our knowledge, in France, no study compared dental monitoring schedules to prevent MRONJ and no cost-effectiveness study has been carried out.
Conclusion
As MRONJ can negatively affect patients' QoL, it is important to determine in a dedicated randomized study, the best dental monitoring schedule for MRONJ prevention. This study suggested that a regular dental follow-up every 4 months may be a suitable option for prevention and early detection/treatment of MRONJ.
Funding
This research did not receive any specific funding.
Authors contribution
S. Beaudouin: had full access to all the data used to generate the study population, conception and design, acquisition, analysis, interpretation, drafting of the manuscript, reviewing, statistical analysis. L-M. Scailteux: Conception and design, acquisition, analysis, interpretation of the data, revision, statistical analysis, administrative, technical, material support and supervision. R. Gamby: Acquisition, analysis and interpretation. S. Cairon-Lejeune: had full access to all the data used to generate the study population, Conception and design, Acquisition, analysis and interpretation, revision, Administrative, technical, or material support and supervision.
Conflicts of interests
The authors declare no conflict of interest.
Informed consent
The authors declare that, according the French regulations, informed consent was obtained from each patient.
Ethical commitee approval
Ethical approval was granted by the University Hospital research ethic committee (#19.140).
Acknowledgements
The authors gratefully acknowledge Dr Triquet Louise, the members of the Eugène Marquis Cancer Institute and of the Dental Care Center for their support in this study.
References
- Bink K. Analysis of denosumab on skeletal-related events in patients with advanced breast cancer. Clin J Oncol Nurs 2015;19:E108–E114. [CrossRef] [PubMed] [Google Scholar]
- Macedo F, et al. Bone metastases: an overview. Oncol Rev 2017:11. DOI: 10.4081/oncol.2017.321. [Google Scholar]
- Domschke C, Schuetz F. Side effects of bone-targeted therapies in advanced breast cancer. Breast Care 2014;9:8. [CrossRef] [Google Scholar]
- Hanley DA, Adachi JD, Bell A, Brown V. Denosumab: mechanism of action and clinical outcomes. Int J Clin Pract 2012;66:1139–1146. [CrossRef] [PubMed] [Google Scholar]
- Henry DH, et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol 2011;29:1125–1132. [CrossRef] [PubMed] [Google Scholar]
- Nicolatou-Galitis O, et al. Medication-related osteonecrosis of the jaw: definition and best practice for prevention, diagnosis, and treatment. Oral Surg Oral Med Oral Pathol Oral Radiol 2019;127:117–135. [CrossRef] [PubMed] [Google Scholar]
- Stopeck AT, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010;28:5132–5139. [CrossRef] [PubMed] [Google Scholar]
- Lipton A, et al. Superiority of denosumab to zoledronic acid for prevention of skeletal-related events: a combined analysis of 3 pivotal, randomised, phase 3 trials. Eur J Cancer 2012;48:3082–3092. [CrossRef] [PubMed] [Google Scholar]
- Hayes AR, Brungs D, Pavlakis N. Osteoclast inhibitors to prevent bone metastases in men with high-risk, non-metastatic prostate cancer: a systematic review and meta-analysis. PLOS ONE 2018;13:e0191455. [CrossRef] [PubMed] [Google Scholar]
- Kulkarni AG, Patel A. Denosumab: a potential new treatment option for recurrent aneurysmal bone cyst of the spine. SICOT-J 2019;5:10. [CrossRef] [EDP Sciences] [PubMed] [Google Scholar]
- de Groot AF, Appelman-Dijkstra NM, van der Burg SH, Kroep JR. The anti-tumor effect of RANKL inhibition in malignant solid tumors − a systematic review. Cancer Treatment Rev 2018;62:18–28. [CrossRef] [Google Scholar]
- Uday S, et al. Osteonecrosis of the jaw and rebound hypercalcemia in young people treated with denosumab for giant cell tumor of bone. J Clin Endocrinol Metab. 2018;103:596–603. [CrossRef] [PubMed] [Google Scholar]
- Saad F, et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann Oncol 2012;23:1341–1347. [CrossRef] [PubMed] [Google Scholar]
- Murphy J, Mannion CJ. Medication-related osteonecrosis of the jaws and quality of life: review and structured analysis. Br J Oral Maxillofac Surg 2020;58:619–624. [CrossRef] [PubMed] [Google Scholar]
- Khan A, Morrison A, Cheung A, Hashem W, Compston J. Osteonecrosis of the jaw (ONJ): diagnosis and management in2015. Osteoporosis Int. 2016;27:853–859. [CrossRef] [PubMed] [Google Scholar]
- Otto S, Pautke C, Van den Wyngaert T, Niepel D, Schiødt M. Medication-related osteonecrosis of the jaw: prevention, diagnosis and management in patients with cancer and bone metastases. Cancer Treatment Rev. 2018;69:177–187. [CrossRef] [Google Scholar]
- Pazianas M. Osteonecrosis of the Jaw and the Role of Macrophages. JNCI J Natl Cancer Inst 2011;103:232–240. [CrossRef] [PubMed] [Google Scholar]
- Boquete-Castro A, Gómez-Moreno J, Calvo-Guirado L, Aguilar-Salvatierra A, Delgado-Ruiz RA. Denosumab and osteonecrosis of the jaw. A systematic analysis of events reported in clinical trials. Clin Oral Implants Res 2016;27:367–375. [CrossRef] [PubMed] [Google Scholar]
- Di Fede O, et al. The dental management of patients at risk of medication-related osteonecrosis of the jaw: new paradigm of primary prevention. BioMed Res Int 2018;1–10. [Google Scholar]
- Ruggiero SL, et al. American association of oral and maxillofacial surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J Oral Maxillofacial Surg 2014;72:1938–1956. [CrossRef] [Google Scholar]
- Coleman R, et al. Bone health in cancer: ESMO clinical practice guidelines. Ann Oncol. 2020;31:1650–1663. [CrossRef] [Google Scholar]
- Lettres aux professionnels de santé_Recommandations sur la prise en charge bucco-dentaire des patients traités par bisphosphonates_AFSSAPS2007. Accessed: Jan. 14, 2021. [Online] https://ansm.sante.fr/S-informer/Informations-de-securite-Lettres- aux-professionnels-de-sante/Recommandations-sur-la-prise-en-charge-bucco-dentaire-des-patients-traites-par-bisphosphonates [Google Scholar]
- Société Française de Stomatologie, Chirurgie Maxillo-Faciale et Chirurgie Orale, Ostéonécrose des mâchoires en oromaxillofaciale et traitements médicamenteux à risque (antirésorbeurs osseux, antiangiogéniques)_Recommandations de Bonnes Pratiques-2013. Accessed: Jan. 14, 2021. [Online] http://www.sfscmfco.fr/wp-content/uploads/2012/12/Reco-chirurgie-oromaxillofaciale-et-médicaments-antirésorbeurs.VF-juillet-2013.pdf [Google Scholar]
- Confrère C. Lettre aux professionnels de santé “Denosumab 120mg (XGEVA®): Mise à jour des informations de sécurité d'emploi pour minimiser les risques d'ostéonécrose de la mâchoire et d'hypocalcémie, ”_ANSM2014. https://ansm.sante.fr/S-informer/Informations-de-securite-Lettres-aux-professionnels-de-sante/Xgeva-R-denosumab-nouvelles-informations-pour-minimiser-les-risques-d-osteonecrose-de-la-machoire-et-d-hypocalcemie-Lettre-aux- professionnels-de-sante [Google Scholar]
- Owosho AA, et al. Medication-related osteonecrosis of the jaw: an update on the memorial sloan kettering cancer center experience and the role of premedication dental evaluation in prevention. Oral Surg Oral Med Oral Pathol Oral Radiol 2018;125:440–445. [CrossRef] [PubMed] [Google Scholar]
- Dimopoulos MA, et al. Reduction of osteonecrosis of the jaw (ONJ) after implementation of preventive measures in patients with multiple myeloma treated with zoledronic acid. Ann Oncol 2009;20:117–120. [CrossRef] [PubMed] [Google Scholar]
- Okuma S, Matsuda Y, Nariai Y, Karino M, Suzuki R, Kanno T. A retrospective observational study of risk factors for denosumab-related osteonecrosis of the jaw in patients with bone metastases from solid cancers. Cancers 2020;12:1209. [CrossRef] [Google Scholar]
- Egloff-Juras C, et al. Denosumab-related osteonecrosis of the jaw: a retrospective study. J Oral Pathol Med 2018;47:66–70. [CrossRef] [PubMed] [Google Scholar]
- Khan AA, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Mineral Res 2015;30:3–23. [CrossRef] [Google Scholar]
- Ohga N, Sato J, Asaka T, Morimoto M, Yamazaki Y, Kitagawa Y. Successful conservative treatment of jaw osteonecrosis caused by denosumab in patients with multiple bone metastasis. J Oral Sci 2018;60:159–162. [CrossRef] [PubMed] [Google Scholar]
All Tables
Staging proposed by the American Association of Oral and Maxillofacial Surgeons (AAOMS).
All Figures
|
Fig. 1 Study flowchart. |
| In the text | |
|
Fig. 2 Number of cases of MRONJ in function of denosumab exposure duration (number of injections). |
| In the text | |
|
Fig. 3 Estimated MRONJ-free survival. Times in months. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.