| Issue |
J Oral Med Oral Surg
Volume 29, Number 4, 2023
|
|
|---|---|---|
| Article Number | 42 | |
| Number of page(s) | 6 | |
| DOI | https://doi.org/10.1051/mbcb/2023043 | |
| Published online | 02 February 2024 | |
Case Report
Simultaneous mandibular advancement, maxilla-mandibular all-on-four and immediate loading: a case report
1 Department of oral surgery, University Hospital of Montpellier, Nîmes, France
2
University of Montpellier, School of Dentistry, Montpellier, France
3
Private Maxillo facial and oral surgery clinic, Rodez, France
* Correspondence: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
31
May
2023
Accepted:
6
December
2023
Abstract
Introduction: Full arch reconstruction with dental implants is considered as a reference for dental rehabilitation. However, there are some limitations with patient affected by severe maxilla, mandible atrophy and dento-skeletal-disharmony. These defaults can be corrected with orthognathic surgery and several bone grafts. Observations: A partially edentulous 65-year-old female patient with a skeletal class II by mandibular retrognathia was treated with mandibular advancement osteotomy and simultaneous insertion of four fully guided implants with immediate screwed zirconia prostheses loading in just one session. Conclusion: Simultaneous bilateral sagittal split osteotomy with a full arch rehabilitation by implant with immediate loading by zirconia prosthesis seems to be a reliable and predictable approach to treat skeletal class II patient with a fixed solution. Virtual planning was compulsory to be able to perform this surgery with accuracy.
Key words: Dental implants / mandibular advancement / immediate dental implant loading / computer aided surgery / case report
© The authors, 2023
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Important skeletal class II limits ideal implant placement due to the offset between the maxilla and the mandible. These patients are mainly treated with cantilever fixed prostheses or removable dental prostheses when the cantilever is too important. Bilateral sagittal split osteotomy (BSSO) associated with bone graft is a procedure that can correct this skeletal base discrepancy. However, these protocols usually take several months to be accomplished. Even if the success rate is good, many tools and protocols were developed these past years that allows to greatly reduce treatment time. Such as computer-guided implant surgery, optical impression, virtual orthodontic and 3D printing [1–3].
However, to the best of our knowledge, no authors have described an all in one procedure where the mandibular osteotomy, the bone graft, the implant placement and the immediate loading with a screwed zirconia prosthesis are performed in one surgery.
This article aims to describe our custom method to perform this surgery with a clinical case.
Observation
A 65-year-old female patient was addressed to us for a fixed maxilla and mandible rehabilitation with an aesthetic demand. She had no particular medical history. The patient presented a skeletal and dental class II relationship. The mandible was partially edentulous and there was terminal periodontal disease of both jaws. She also presented facial asymmetry due to the longer left mandibular ramus and condyle with a leftward tilt of the occlusal plane.
The clinical and radiological assessment consisted of several preoperative photos, optical impression of the maxilla and mandible, the recording of the jaw motion and the dynamic occlusion using ModJaw®, a panoramic and cephalometric radiograph, wide field cone beam computed tomography (CBCT) (Fig. 1). The CBCT showed an asymptomatic left condylar hyperplasia. The shade of the tooth and the gum was recorded by the prosthetist at the practice.
After a complete review, the patient was proposed: a fixed rehabilitation on maxillo-mandibular double all-on-four implants with a mandibular advancement to correct the skeletal class II, the occlusal tilt and the vertical asymmetry and an instant loading with two zirconia bridges in a single surgery.
Using coDiagnostiX® and DWOS® we were able to simulate the BSSO, the virtual placement of the implants and to model the future prostheses. Based on the simulation we generated the custom splint for the BSSO and the custom home-designed titanium guides for drilling and subsequent implant placement. The guide was bone supported and fixed with screws (Figs. 2 and 3).
The surgical intervention was performed under general anesthesia. The first step was to extract a traumatically the remaining teeth at the mandible and the maxilla. Then a crestal incision was realized along the entire length of the maxilla with two posteriors release incisions. A full-thickness flap was elevated. At this point, the guide was set up, this was a critical and time-consuming step because the whole surgery depends on the implant positioning. Once the guide has been fixed with screws, we started the drilling sequence based on a modified Straumann® protocol to enhance our drill precision. Then we placed the four implants through our guide. The same procedure is performed at the mandible (Fig. 4).
We tried to get the highest tightening torque possible on each implant. All implants were Straumann®BLX®SLA® regular base.
Afterwards, the immediate loading with the two zirconia prostheses of the implants was performed; several orthodontic buttons were bonded to the ceramic preoperatively. Then an Epker BSSO was performed using a piezo surgical device. This part of the surgery was similar to a classical mandibular advancement: osteotomy, bilateral split, maxillo-mandibular fixation, osteosynthesis and unlocking. The osteosynthesis was performed using one plate on each side. After the unlocking, we checked the occlusion based on the simulation (Fig. 5). The gap between the segments was filled with allogeneic bone graft (Biobank®), in every socket, and on the buccal side of implants with xenograft bone graft (Xenograft-Straumann®).
Finally, we did the sutures with polytetrafluoroethylene and resorbable thread. The vestibular and lingual flap is sutured over the zircon, coronary pulled up like in gum graft, leaving the part below the prostheses on directed wound healing. Postoperatively, the occlusion was controlled with class II elastics hooked on the orthodontics buttons for two months.
The postoperative instructions were to eat soft food during 2 months. The treatment was 7 days of amoxicillin, 4 days of corticosteroids, analgesics and mouth rinse.
We saw the patient afterward at 7 days to screw again the prostheses, 21 days to remove sutures and 3 months to check the implants with the Implant-Stability-Quotient (ISQ). At each postoperative appointment, the occlusion was modified by adjusting the zircon (Fig. 6). The patient had physiotherapist sessions to reeducate the jaw and to learn new masticatory functions in the meantime.
 |
Fig. 1 (a) preoperative endobuccal view (b) panoramic: preoperative clinical situation. |
 |
Fig. 2 (a) Mandibular prosthesis and implants simulation (b) Maxillary prosthesis and implant simulation. |
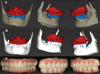 |
Fig. 3 (a) Occlusion simulation before mandibular advancement (b) Occlusion simulation after Mandibular Advancement and rotation (c) Glazed Machined Zirconia prosthesis. |
 |
Fig. 4 (a) Fixed maxillary and (b) mandibular guide and implants. |
 |
Fig. 5 Occlusion (a) before and (b) after the osteotomy. |
 |
Fig. 6 3 Months postoperative (a) panoramic; (c) prosthesis front view; (b) Maxillary gingiva; (D) Mandibular gingiva; Front picture (e) before and (f) after surgery. |
Discussion
BSSO with mandibular advancement is a successful method to correct the maxillo-mandibular shift. This procedure is mainly used in dentulous mandible. Reconstructing edentulous patient, sagittal discrepancy represents a challenge for fixed solutions. This gap can be increased with the centripetal resorption of the bone due to premature teeth extraction [4]. Currently, a prosthesis can balance a sagittal bone discrepancy of 4/5 mm without any loading problems in terms of cantilever. In case of greater sagittal maxillo-mandibular gaps, a prosthetic compensation could lead to implant or prosthesis failure, patient discomfort due to a high prosthesis volume, even aesthetic problems and difficulty in maintaining sub-prosthetic hygiene.
Nowadays, patients frequently request a functional and aesthetic oral rehabilitation with the shortest possible treatment duration, with immediate results and maximum comfort. Many techniques were described to treat jaw atrophy. The common goals of these protocols are: treatment time reduction, avoiding bone graft harvesting and to perform the immediate implant loading [3].
No case reports or articles combining those concepts to rehabilitate edentulous patients with skeletal class II were found in our literature research. We only founded some articles with simultaneous Le Fort I osteotomy, zygomatic implants and immediate loading in patient presenting a skeletal class III [5–7].
To create a procedure that can correct the skeletal discrepancy and improve the implant placement to avoid cantilever at the mandible and considering patients' complaints, computer-assisted surgery is necessary. Several softwares were used (coDiagnostiX®, Meshmixer®, DWOS®) to model the surgical guide. Rigid and bone supported guide is necessary to be able to performed an immediate loading by a screwed prosthesis. Additional zircon sleeves were used to gain precision for our implants placing (Fig. 4). The original Straumann® sleeve is not perfectly adjusted to the implant holder. Moreover, this allows the implant to be guided from the very start. This method requires a different thinking process that can be difficult to learn and is time consuming.
In an edentulous mandible, the surgical approach for mandibular advancement is different. Anatomical landmarks and bone quality are not the same as in conventional class II BSSO. An Epker BSSO was performed. A longer proximal segment allows for a larger bone contact reducing pseudarthrosis risks. Good experience in conventional mandibular advancement is necessary.
From our perspective this procedure had an excellent result regarding, aesthetic, function and precision. The patient was also very satisfied by this intervention. To this day, no implants failed in our orthognathic/dental implant surgery. However, Kim et al. [8,9] theorize that orthognathic surgeries might impair the osteointegration of dental implants due to regional acceleratory phenomenon (RAP) with more marginal bone loss, a diminished ISQ and implant success. RAP is an acute inflammatory phase and intense osteoclastic bone resorption, which manifests as transient local osteopenia combined with decreased osteoblastic bone formation [10,11]. Nevertheless, the physiopathology of this phenomenon is not fully understood, there is no scientific consensus on how RAP is modifying the surrounding tissue and how it could affect implants osteointegration. Randomized control trials are needed to confirm or to refute this hypothesis.
Conclusion
Simultaneous BSSO with a full arch rehabilitation by implant with immediate loading by zirconia prosthesis seems to be a reliable and predictable approach to treat skeletal class II patient with a fixed solution. More follow-up will be necessary to validate this procedure. Virtual planning, experiences in more classical protocols and a good cooperation between the surgeon and the prosthetist are necessary to be able to achieve this precision of surgery.
Conflict of interest
The authors declare that they have no competing interest.
Funding
This research did not receive any specific funding.
Ethical approval
Ethical approval was not required.
Informed consent
Written informed consent was obtained from the patient.
Authors contributions
P. Ba Lam: writing, editing; P. Dimitri: main operator, editing, reviewing.
References
- Gargallo-Albiol J, Barootchi S, Marqués-Guasch J, Wang H-L. Fully guided versus half-guided and freehand implant placement: systematic review and meta-analysis. Int J Oral Maxillofac Implants 2020;35:1159–1169. [CrossRef] [PubMed] [Google Scholar]
- Laleman I, Bernard L, Vercruyssen M, Jacobs R, Bornstein MM, Quirynen M. Guided implant surgery in the edentulous maxilla: a systematic review. Int J Oral Maxillofac Implants 2016;31:s103–s117. [Google Scholar]
- Lerner H, Hauschild U, Sader R, Ghanaati S. Complete-arch fixed reconstruction by means of guided surgery and immediate loading: a retrospective clinical study on 12 patients with 1 year of follow-up. BMC Oral Health 2020;20:15. [CrossRef] [PubMed] [Google Scholar]
- Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral Maxillofac Surg 1988;17:232–236. [CrossRef] [PubMed] [Google Scholar]
- Grecchi F, Grecchi E, Del Fabbro M, Goker F. Simultaneous Le Fort I osteotomy and zygomatic implant placement. J Cranio-Maxillofac Surg 2022;50:114–123. [CrossRef] [Google Scholar]
- Goker F, Grecchi E, Del Fabbro M, Grecchi F. Oral rehabilitation of bilateral cleft lip and palate patient with simultaneous LeFort I osteotomy and zygomatic implants: a case report. Cleft Palate-Craniofacial J 2022;59:1433–1438. [CrossRef] [PubMed] [Google Scholar]
- Grecchi F, Zollino I, Parafioriti A, Mineo G, Pricolo A, Carinci F. One-step oral rehabilitation by means of implants' insertion, Le Fort I, grafts, and immediate loading. J Craniofac Surg 2009;20: 2205–2210. [Google Scholar]
- Kim J-W, Lee H, Lim H-K, Kim J-W, Byun S-H, Choi Y-J, et al. Orthognathic surgery Deteriorates the osseointegration of dental implants: a propensity-matched multicentre cohort study. J Oral Rehabil 2018;45:967–973. [CrossRef] [PubMed] [Google Scholar]
- Kim J, Kim H, Kim S, Kim S. Impaired osseointegration of dental implants associated with orthognathic surgery: possible regional acceleratory phenomenon. Clin Implant Dent Relat Res 2019 cid. 12745. [Google Scholar]
- Liou EJW, Chen P-H, Wang Y-C, Yu C-C, Huang CS, Chen Y-R. Surgery-first accelerated orthognathic surgery: postoperative rapid orthodontic tooth movement. J Oral Maxillofac Surg 2011; 69:781–785. [CrossRef] [PubMed] [Google Scholar]
- Feller L, Khammissa RAG, Siebold A, Hugo A, Lemmer J. Biological events related to corticotomy-facilitated orthodontics. J Int Med Res 2019;47:2856–2864. [CrossRef] [PubMed] [Google Scholar]
All Figures
|
Fig. 1 (a) preoperative endobuccal view (b) panoramic: preoperative clinical situation. |
| In the text | |
|
Fig. 2 (a) Mandibular prosthesis and implants simulation (b) Maxillary prosthesis and implant simulation. |
| In the text | |
|
Fig. 3 (a) Occlusion simulation before mandibular advancement (b) Occlusion simulation after Mandibular Advancement and rotation (c) Glazed Machined Zirconia prosthesis. |
| In the text | |
|
Fig. 4 (a) Fixed maxillary and (b) mandibular guide and implants. |
| In the text | |
|
Fig. 5 Occlusion (a) before and (b) after the osteotomy. |
| In the text | |
|
Fig. 6 3 Months postoperative (a) panoramic; (c) prosthesis front view; (b) Maxillary gingiva; (D) Mandibular gingiva; Front picture (e) before and (f) after surgery. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.