| Issue |
J Oral Med Oral Surg
Volume 29, Number 4, 2023
|
|
|---|---|---|
| Article Number | 39 | |
| Number of page(s) | 6 | |
| DOI | https://doi.org/10.1051/mbcb/2023040 | |
| Published online | 23 January 2024 | |
Technical Note
Zygomatic implants under local anesthesia: A technical note
1
Maxillofacial surgery department. CHU Hotel Dieu, Nantes
2
Hospital practice, Maxillofacial Surgery Department, CHU Hotel Dieu, Nantes
* Correspondence : This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
14
April
2023
Accepted:
4
October
2023
Abstract
The placement of zygomatic implants is a surgical procedure that is most often performed under general anesthesia, due to the duration and the difficulty of the procedure, and in particular due to the necessity of a significant detachment. However, depending on the operator's experience, this procedure can be performed under local anesthesia. Indeed, this variation offers many advantages. It simplifies the procedure, allows the patient's collaboration as well as a radiological control during the operation and reduces the postoperative effects. It also eliminates any risk related to general anesthesia. It is systematically practiced in our activity with a very good acceptance from the patients.
Key words: Zygomatic implants / alveolar bone loss / local anesthesia / oral surgery / dental implants
© The authors, 2023
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
The indications for zygomatic implants are reserved for extreme maxillary atrophy as an alternative to bone grafts [1,2]. Thanks to their zygomatic cortical anchorage, these implants provide good primary stability and allow for immediate loading with a temporary bridge [3]. This is an undeniable advantage of this technique compared to bone grafting, and it often wins over patients. According to a recent systematic review of the literature, zygomatic implants have a high long-term survival rate (96.5% with an average of 91.5 months of follow-up), with no significant difference compared to conventional implants [4]. However, the indications must be well supervised because of the risk of long-term complications with zygomatic implants [4]. Standard practice involves resorting to general anesthesia. The use of general anesthesia is widely accepted in the articles published since the development of the zygomatic implant technique [5]. Thus, performing this surgery under general anesthesia allows for a more extensive soft tissue detachment, allowing for good visualization and therefore better visual control of the axis, and the exit point of the zygomatic implant apex. This could certainly minimize complications such as effraction of the orbit [6,7] or the infratemporal fossa. Finally, general anesthesia can also greatly facilitate surgery in cases of strong gag reflex, poor lip laxity, or for excessively stressed patients. However, the use of general anesthesia raises a number of challenges detailed thereafter.
In this work, we present an alternative framework, based on local anesthesia that considerably reduces patient discomfort and costs while presenting similar outcomes.
Innovation report
In our practice, we report 25 patients who received 54 zygomatic implant placements under local anesthesia between 2019 and 2022. The average age of this sample was 66.3 yr.
Conditioning of the patient
The indication of zygomatic implants was established during the initial consultation, using the clinical examination and CBCT imaging. A careful examination of the patient's medical history and treatments was done. Known allergies and smoking history were noted. Half of the patients had no general medical history and were not taking any treatment, 12% were treated with antiplatelet agents or anticoagulants, 16% were treated for hypothyroidism and 4% of the patients were smokers. Then, extraoral and intraoral examinations were performed. Photographs and impressions were made.
This first consultation aimed to make the procedure under local anesthesia part of a routine and well-protocolised practice, in order to minimize the impressiveness of the procedure. The additional complexity brought by the placement of zygomatic implants was presented as a painless procedure that is well tolerated by the patients, without minimizing the difficulty of the drilling. The patients' fears were always taken into account and were reduced by prescribing a premedication. A combination of alprazolam 0,5 mg and hydroxyzine 50 mg (adapted according to morphology) was prescribed, and needed to be taken 1h30 before the surgery. Anxiolytics were taken by 64% of the patients treated with this technic.
Nevertheless, depending on the context and the request, the use of general anesthesia was not ruled out. It was necessary to contraindicate a local anesthesia in extreme cases, notably syndromic cases of sequelae of cleft lip and palate due to the low laxity of the lips.
A radiographic planning was made using the BlueSkyPlan® software (Fig. 1). It was necessary in order to choose the optimal length, direction, and position of the zygomatic implants according to the thickness of the zygomatic bone, the alveolar height of the remaining bone, and the planned prosthetic rehabilitation.
 |
Fig. 1 Radiographic planning of implants. |
Surgery
The procedure took place in a clean room dedicated to surgery and the patient was advised not to fast. For each surgery, the medical room was equipped with a complete first-aid kit as well as a blood pressure monitor and a defibrillator, in order to cover all eventualities. Of the 25 patients treated, 4 patients received a quad zygoma (16%) and 21 patients received a hybrid zygoma (84%).
The anesthesia was done by endobuccal way only with injections of articaine 40 mg/mL hydrochloride adrenalized 1/100000. 4 to 8 carpules of 1,8 mL were used per surgery, depending on the patient's needs. Nerve blocks were performed at the level of the infraorbital foramens and the anterior aspect of the zygomatic bones was anesthetized through the bottom of the maxillary vestibule (Fig. 2). Nerve blocks were also performed at the palatal foramen and at the retroincisal foramen (Fig. 3). The crestal incision was extended by posterior vestibular discharges going up to the first molars along the maxillo-zygomatic arch. Subperiosteal roughening was performed along this arch and the anterior aspect of the zygoma. It aimed to free the masseter muscle attachments. It should be noted that unlike a procedure performed under general anesthesia, the detachment in this case was much more restricted and limited only to the area of interest (Figs. 4 and 5), in order to simplify the postoperative course. In the case of hybrid zygomas, it was not necessary to expose the infraorbital foramen. Then, when needed, patients underwent one or more multiple implant or dental avulsions (approximately 60% of the patients). A few patients received anterior bone resection (16%). The drilling phase was the critical phase because it was the one that required the most attention from the operator, but which could cause the most stress for the patient. The patients were warned and reassured about the advent of vibrations and noises during this phase of the surgery. Gestures were performed gently to improve comfort. When needed, a per-operative radiological check-up (cone-beam computed tomography) was performed during the surgery (Fig. 6), especially in cases of quad zygomas, when the anterior implant could be sometimes close to the orbit and where there could be a poor visibility and possibility of an orbital concavity. To avoid making a complete breakthrough through the sinus floor, the implants were positioned extramaxillary, resting on the anterior wall of the sinus (Fig. 7). An intra-sinusal position could have increased the risk of chronic sinusitis. Cheek fat pad flaps were performed for 88% of the patients at the end of the surgery, in order to cover and protect the implant necks (Fig. 8). For one patient, transposition of the cheek fat pad was used to close an oral-sinus communication.
Two patients received filling with drill bone vestibular to the implants. It was also necessary to resect keratinized gingiva in one patient. Sutures using separate stitches on the vertical releasing incisions and continuous stiches on the crest were performed at the end of the surgery. For one patient, a mandibular all on 6 was performed in the same surgery as the maxillary hybrid zygomas.
For all patients, the implant positioning impressions were made immediately after surgery. Impressions were made with the help of photogrammetry for the implant's positions and a digital impression of the mucosa or with an open tray technic using the hollowed out prosthesis.
A seven-day course of antibiotics (amoxicillin 1 g, 2 times a day, or, in case of allergy, clindamycin 600 mg, 2 times a day) was prescribed, and paracetamol (1 g) three times daily for three days, and 0.2% chlorhexidine mouth wash were used. Standard postoperative instructions were given to the patients including oral hygiene measures, refraining from smoking, avoidance of nose blowing, and forceful mouth rinsing for ten days postoperatively.
Patients were followed up after 2 days, two weeks, 1 month and 4 months to assess postoperative complications.
 |
Fig. 2 Areas of infiltration of local anesthetic (vestibular view). |
 |
Fig. 3 Areas of infiltration of local anesthetic (palatal view). |
 |
Fig. 4 Differences between subperiosteal detachments under general anesthesia (left) and under local anesthesia (right). |
 |
Fig. 5 View of the subperiosteal detachment under local anesthesia. |
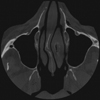 |
Fig. 6 Cone beam computed tomography per-operative control. |
 |
Fig. 7 View of the extramaxillary implants. |
 |
Fig. 8 View of the cheek fat pad flap. |
Complications
Minimal surgical complications were recorded. One perforation of the Schneiderian membrane was noted. Postoperatively, minimal oedema and bruising were noted, and none of the patients developed any alteration in sensation related to the cheek or the nose.
The complications found in our experience were not related to the use of local anesthesia. There were two cases of postoperative hemorrhage in 72- and 73 yr old patients under rivaroxaban, with sutures being done again the same day. One patient fractured a right multi-unit abutment screw twice, due to poor implant positioning away from the bone crest. The mechanical stresses put strain on the abutment and fractured the screw. This implant was mobile at its neck in all three planes of space. This same patient also presented with cellulitis on the side of the zygomatic implant, which was also a complication related to implant positioning.
Two patients presented partial necrosis of the cheek fat pad, which led to gingival recession in one of the patients. Two patients presented episodes of infectious-looking cheek edema that regressed with antibiotics, which may be related to contamination of the cheek fat pad by bacteria of oral origin.
Postoperative swelling at the palatal level occurred for one patient, while another patient presented an inflammation around the pillars at 2 months after the surgery, although he had good oral hygiene. This was probably related to a reaction to the resin of the bridge, but gradually decreased afterwards. Another patient presented at the 4-month postoperative check-up with inflammation around a zygoma implant neck due to a lack of keratinized gingiva. No patient reported sinusitis.
Two patients reported discomfort in the cheekbones due to the apex of a zygomatic implant. The other complaints reported by the patients concerned the prosthesis (aesthetic complaint for one patient and difficulty biting for one patient).
Osseointegration was achieved in all cases except one on a hybrid zygomas case. The patient had hypothyroidism and his zygomatic bone was very thin and the bone density was low allowing a very low primary stability of the implant (15 N). At the 6-month follow-up, the implant was removed. All patients proceeded to the prosthetic rehabilitation phase.
Discussion
There are few articles in the literature dealing with the placement of zygomatic implants under local anesthesia. It can be noticed that the different studies related to zygomatic implants focus on surgical techniques, implant and prosthetic success rates, as well as short and long-term complications. The use of local anesthesia (LA) makes it easy to perform intraoperative and immediate postoperative control imaging, which can facilitate implant placement, and avoid complications such as intra-orbital effraction. The cooperation of the patients allows them to open their mouth spontaneously, which simplifies the procedure considerably compared to general anesthesia. Furthermore, we have seen in our practice that the minimal detachment achieved allows for better postoperative follow-up (less edema and postoperative pain). The discomfort linked to nausea, the throat pain linked to intubation and hospitalization are also avoided. For patients, having the procedure performed in an ambulatory clinic reduces the expense of the hospital procedure and allows them to go home soon after the surgery, provided they are operated on by experienced professionals [8].
Another advantage of local anesthesia is that it makes it easier and more reproducible to take the patient's occlusion during the impression at the end of the procedure. However, the decreased mouth opening at the end of the procedure can compromise the impression taking.
Controlling the patient's stress and anxiety is a key factor in the feasibility of such a surgery under local anesthesia. Indeed, the vibrations caused as well as the proximity of structures such as the orbit can be embarrassing for the patient. The prescription of an anxiolytic premedication can be one of the solutions to this problem. A case series of 29 patients from 2014 shows the use of premedication with midazolam (7.5 mg to 15 mg orally) 1 h before zygomatic implant surgery under LA [9]. Another case series also shows the use of intravenous sedation combined with local anesthesia. The authors used a combination of IV diazepam (15 mg) and IV meperidine (75 to 100 mg) [10]. A retrospective cohort [8] compares the use of general anesthesia (group 1), local anesthesia with intravenous sedation (combination of Diazepam 10 mg/Midazolam 10 mg) (group 2), and local anesthesia with sedative premedication (midazolam 15 mg) (group 3). Local anesthesia with sedative premedication was used only in short surgery with very experienced surgeons, on 3 patients. Almeida et al. [8] showed no significant difference in the satisfaction of individuals subjected to general anesthesia, or local anesthesia with sedation, on all the aspects analyzed.
Stress and anxiety management could be achieved with alternative non-medicinal techniques such as the use of virtual reality [11]. However, for the time being, the clutter of the virtual reality headset would greatly hinder the performance of this surgery. Perhaps the evolution of the equipment will facilitate its use in this type of surgery.
Finally, techniques such as navigated surgery or guided surgery allow less experienced practitioners to perform this type of surgery, or for complex cases (zygomatic atrophy, quad zygomas), thus facilitating the use of local anesthesia [12]. A recent article describes the use of this flapless technique via navigated surgery on patients under local anesthesia, to obtain minimal postoperative effects [13]. In addition, with the advent of the extramaxillary technique for placing zygomatic implants [14], in which the zygomatic implants are placed outside the maxillary sinus, the surgical time is reduced. It allows the surgical procedure to be performed in an outpatient clinic under local anesthesia and sedation, for immediate or delayed loading [15,16].
We have noted an evolution in our practice. Initially, the indications for zygomatic implants under local anesthesia were only in cases where a single zygomatic implant was placed. Nowadays, 90% of zygomatic implants are realized under local anesthesia in our practice. Prescriptions for preoperative sedation are now much more systematic due to the protocolisation of our practice.
Conclusion
The zygomatic implant technique provides a reliable, long-lasting and comfortable solution for patients. Its practice under local anesthesia allows its democratization and simplification from all points of view. It is very well accepted by patients and has the enormous advantage of being able to perform a peroperative radiological control. It also simplifies the post-operative follow-up in a significant way. This is why it is the first choice for the placement of these implants. However, it requires good experience on the part of the surgeon, who may have recourse to general anesthesia when learning the technique.
Conflict of interest
The author declares a teaching contract for the Nobel Biocare company.
Funding
This research did not receive any specific funding.
Ethical approval
Ethical approval was not required.
Informed consent
Written informed consent was obtained from all patients and/or families.
Authors contributions
Dr Mathilde Nicolas: Concept/Design, Data analysis/interpretation, Drafting article, Statistics, Data collection Dr Julien Guiol: Design, Critical revision of article, Approval of article.
References
- Bedrossian E, Stumpel L, Beckely ML, Indresano T. The zygomatic implant: preliminary data on treatment of severely resorbed maxillae. A clinical report. Int J Oral Maxillofac Implants. 2002;17:861–865. [Google Scholar]
- Malevez C, Abarca M, Durdu F, Daelemans P. Clinical outcome of 103 consecutive zygomatic implants: a 6–48 months follow-up study. Clin Oral Implants Res. févr 2004;15:18–22. [CrossRef] [PubMed] [Google Scholar]
- Davó R, Felice P, Pistilli R, Barausse C, Marti-Pages C, Ferrer-Fuertes A, et al. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 1-year post-loading results from a multicentre randomised controlled trial. Eur J Oral Implantol. 2018;11:145–161. [Google Scholar]
- Moraschini V, de Queiroz TR, Sartoretto SC, de Almeida DCF, Calasans-Maia MD, Louro RS. Survival and complications of zygomatic implants compared to conventional implants reported in longitudinal studies with a follow-up period of at least 5 years: a systematic review and meta-analysis. Clin Implant Dent Relat Res. févr 2023;25:177–189. [CrossRef] [PubMed] [Google Scholar]
- Candel-Martí E, Carrillo-García C, Peñarrocha-Oltra D, Peñarrocha-Diago M. Rehabilitation of atrophic posterior maxilla with zygomatic implants: review. J Oral Implantol. 20 oct 2012;38: 653–657. [CrossRef] [PubMed] [Google Scholar]
- Krauthammer M, Shuster A, Mezad-Koursh D, Shlomi B, Stolovitch C, Leibovitch I. Extraocular muscle damage from dental implant penetration to the orbit. Am J Ophthalmol Case Rep. avr 2017;5: 94–96. [Google Scholar]
- Van Camp P, Vrielinck L, Gemels B, Politis C. Intraorbital hemorrhage following a secondary intervention at integrated zygomatic implants: a case report. Int J Surg Case Rep. 2018;43:21–24. [CrossRef] [Google Scholar]
- Almeida PHT, Salvoni AD, França FMG. Evaluation of satisfaction of individuals rehabilitated with zygomatic implants as regards anesthetic and sedative procedure: A prospective cohort study. Ann Med Surg. oct 2017;22:22–29. [CrossRef] [Google Scholar]
- Rodríguez-Chessa JG, Olate S, Netto HD, Shibli J, de Moraes M, Mazzonetto R. Treatment of atrophic maxilla with zygomatic implants in 29 consecutives patients. Int J Clin Exp Med. 2014;7: 426–430. [Google Scholar]
- Bedrossian E, Rangert B, Stumpel L, Indresano T. Immediate function with the zygomatic implant: a graftless solution for the patient with mild to advanced atrophy of the maxilla. Int J Oral Maxillofac Implants. 2006;21:937–942. [Google Scholar]
- Falguière A, LeGruiec C, Herry H, Genest-Beucher S, Dessus JM, Boisramé S. Contribution of virtual reality in oral surgery: a literature review. J Stomatol Oral Maxillofac Surg. 2021;122: 405–410. [CrossRef] [Google Scholar]
- Ramezanzade S, Keyhan SO, Tuminelli FJ, Fallahi HR, Yousefi P, Lopez-Lopez J. Dynamic-assisted navigational system in zygomatic implant surgery: a qualitative and quantitative systematic review of current clinical and cadaver studies. J Oral Maxillofac Surg. 2021;79:799–812. [CrossRef] [Google Scholar]
- Bhalerao A, Marimuthu M, Wahab A, Ayoub A. Dynamic navigation for zygomatic implant placement: a randomized clinical study comparing the flapless versus the conventional approach. J Dent. 2023;130:104436. [CrossRef] [Google Scholar]
- Aparicio C, Manresa C, Francisco K, Claros P, Alández J, González-Martín O, et al. Zygomatic implants: indications, techniques and outcomes, and the Zygomatic Success Code. Periodontol 2000. 2014;66:41–58. [CrossRef] [PubMed] [Google Scholar]
- Agliardi EL, Romeo D, Panigatti S, de Araújo Nobre M, Maló P. Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: a prospective clinical study with minimum follow-up of 6 years. Int J Oral Maxillofac Surg. 2017;46:1592–1599. [CrossRef] [Google Scholar]
- Araújo R, Sverzut A, Trivellato A, Sverzut C. Retrospective analysis of 129 consecutive zygomatic implants used to rehabilitate severely resorbed maxillae in a two-stage protocol. Int J Oral Maxillofac Implants. 2017;32:377–384. [CrossRef] [Google Scholar]
All Figures
|
Fig. 1 Radiographic planning of implants. |
| In the text | |
|
Fig. 2 Areas of infiltration of local anesthetic (vestibular view). |
| In the text | |
|
Fig. 3 Areas of infiltration of local anesthetic (palatal view). |
| In the text | |
|
Fig. 4 Differences between subperiosteal detachments under general anesthesia (left) and under local anesthesia (right). |
| In the text | |
|
Fig. 5 View of the subperiosteal detachment under local anesthesia. |
| In the text | |
|
Fig. 6 Cone beam computed tomography per-operative control. |
| In the text | |
|
Fig. 7 View of the extramaxillary implants. |
| In the text | |
|
Fig. 8 View of the cheek fat pad flap. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.